


Background
Fragile X syndrome (FXS) is a non-Mendelian nucleotide repeat condition, which is due to the loss of function of the FMR1 (Fragile X Mental Retardation 1) gene. The FMR1 gene is found on the Xq27.3 chromosome and encodes the FMRP protein, which controls the translation of specific messengers. The repetition of CGG triplets (> 200 repetitions) and the promoter’s methylation lead to the gene’s silencing. However, the biological mechanism responsible for the presentation of the SXF is still unknown.1
This syndrome is caused by the hypermethylation of CGG (cytosine-guanine triplet-guanine) repeats, expanded adjacent to exon 1 of the FMR1 gene; this mutation affects more than 98% of people with FXS.2 It is estimated that the disorder affects 1/4,000 men and 1/8,000 women in the general Caucasian population, with 60% of individuals with the complete mutation also having autism spectrum disorders.3 Carriers of fragile X premutation (55-200 CGG repeats) are relatively common in the general population.4
As mentioned above, the FMR1 gene is mapped on the X chromosome at the q27.3 position and encompasses approximately 40 kb of genomic sequence. This gene contains 17 exons, and its mRNA is 4 kb long. Exons 12, 14, 15, and 17 can be spliced alternately, resulting in different mRNA and protein isoforms.5
Fragile X premutation is associated with two clinical disorders: fragile X-associated tremor/ataxia syndrome (FXTAS) and fragile X-associated primary ovarian insufficiency disorder (FXPOI).6 Women who are carriers of premutation may have a spectrum of ovarian dysfunction and may also have normal menstruation with normal or high FSH but with reduced fertility.7
Clinical Case
35-year-old patient. Consulted for primary infertility of 1 year of evolution, relevant biochemical studies were requested, among within the result of Anti-Mullerian Hormone of 0.40 ng/mL, by age and diagnosis of low ovarian reserve it is decided to perform FMR1 mutation analysis in search of the cause of the probable primary ovarian failure, resulting in a premutation with repetition of 49 CGG.
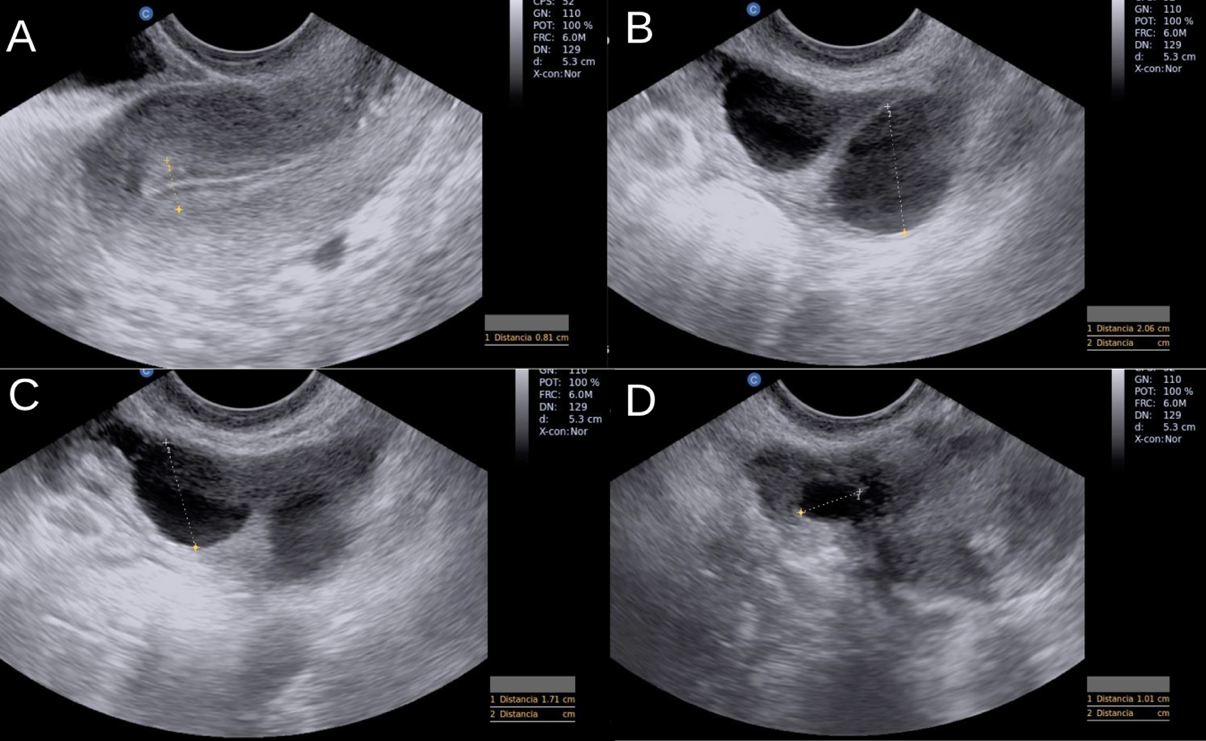
We decide on high-complexity treatment (IVF/ICSI) to increase the chances of pregnancy, using menotropins 300 IU every 24 hours plus dihydrogesterone 30mg orally, as well as the use of testosterone 50 mg transdermal every 24 hours to improve the ovarian response starting from 3rd day of the menstrual cycle. An endocavitary ultrasound was performed on day 11 of the cycle (IMAGE 1). Subsequently, a serum sample of estradiol and progesterone was taken, resulting in 1010.14 pg/ml and 0.63 ng/ml, respectively. Final oocyte maturation was performed with hCG 10,000 IU. Oocyte capture is carried out at 34 hours after day 13 of the cycle, obtaining 4 oocytes being 2 MII; due to the poor response, vitrification of the oocytes obtained was proposed (IMAGE 2), and carrying out from another cycle of ovarian stimulation controlled to obtain more mature oocytes and perform ICSI.
**_endometrial_thickness_8_mm_with_a_tr.png)
.png)
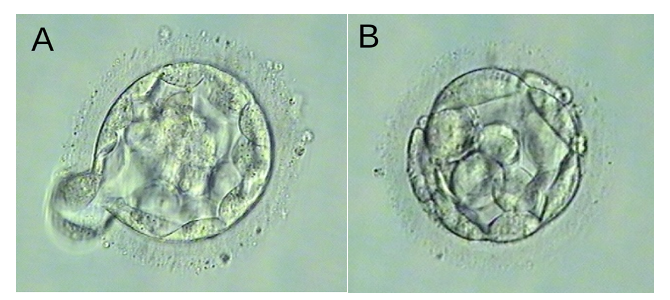
The use of testosterone 50 mg transdermal every 24 hours was continued without suspending it for 2 months, during which the ovarian stimulation cycles were performed, a change of controlled ovarian stimulation was decided because of the patient’s desire and reasons she had to leave the country, a fresh transfer was decided, a second controlled ovarian stimulation was performed with flexible GnRH antagonist protocol, starting on the 3rd day of the cycle using menotropins 300 IU every 24 hours, with GnRH antagonist to inhibit LH peak starting on day 7 of the cycle, on day 10 of the cycle, estradiol and progesterone were taken with the following result Estradiol: 878.82 pg/ml Progesterone: 0.71 ng/ml. Oocyte maturation with hCG 10,000 IU, oocyte capture was carried out on the 14th of the cycle, 34 hours after the trigger, obtaining 4 oocytes being the 4 MII, ICSI was carried out to 6 oocytes in total MII and developing 4 embryos in blastocyst stage ( IMAGE 3 and 4), complying with the criteria of Gardner’s classification according to which a fresh embryo transfer of 1 embryo with BHi AA quality was carried out ( IMAGE 5), vitrifying 3 embryos, 2 with BHi AA quality and one embryo with BHi BA quality (TABLE 1).
**_hatching_blastocyst._**b)**_cavited_blastocyst_of_the_devitrified_oocyte_cycle_(300x.png)
.png)
.png)
Quantification of hCG beta fraction 10 days after embryo transfer, which was 50 mIU/mL, 3 weeks after, endovaginal ultrasound was performed, finding a fetal heart rate of 170 beats per minute. Fetal DNA at 10 weeks of gestation results negative for chromosomal alterations such as trisomy 21, 18, and 13, reporting male sex.
The first-trimester ultrasound was performed by a maternal-fetal doctor, with a screening report for structural alterations without pathological findings; the calculation of risks for chromosomopathies (T.21, T.18, T.13) was considered out of range by caudal skull length (CN) >84 mm. Emerging markers were evaluated, finding them normal, the calculation of risk of placental ischemic syndrome (preeclampsia 1:516, fetal growth restriction 1:587) was considered low, risk of preterm birth of 1:2.965 before the 34 weeks, the calculation of risks of gestational diabetes was counted at 1:24, so from the 24- 28 weeks it was recommended to perform an oral glucose tolerance curve of 75 (CTOG 75). Likewise, organ structural ultrasound was performed by a maternal-fetal doctor at 22 weeks, finding exposed in TABLE 2.
The pregnancy was resolved by cesarean section at 39 weeks of gestation. This resulted in a live male newborn weighing 4,010 kg and a height of 58 cm. Apgar was born on 9/9 without complications.
Materials and Methods
A search was carried out in the Medline database via PubMed using the following terms: “Ovarian insufficiency,” “FXPOI,” “FMR1”, “Female reproductive health,” and “CGG repeat.” The following filters limited the search: “Case Reports,” “Review,” “Systematic Reviews”, and “Books and Documents,” “Spanish and English”, from 1981 to 2021, in total 1,978 studies were found, editorials, reviews, duplicate articles were excluded, and 33 studies were selected that included women with primary ovarian insufficiency associated with the premutation of the FMR1 gene.
Discussion
Transcriptional silencing of FMR1 results in the loss of the fragile mental retard protein X (FMRP), which is necessary for neuronal development and cognition. Carriers of FMR1 premutation also have disorders associated with ovarian function, including loss of fertility and hypoestrogenic (FXPOI), as well as neurodegeneration with associated memory loss and general Parkinsonism (FXTAS).8
Biological Bases of Fragile X Syndrome
The exact biological mechanism responsible for the presentation of SXF is unknown; however, it is known to lie in the ability of the FMRP protein to bind to RNA and proteins. Specifically, FMRP joins ribosomes and is present in the synaptic compartments, which control the translation of specific messengers. The loss of FMRP causes alterations in synaptic connectivity in neurons, translating into the specific symptoms of SXF. These synaptic connectivity alterations manifest in the brain with the decrease in the number of dendrites and spines in the neurons of patients with FXS.1
The lack of FMRP in neurons leads to an exacerbated expression of glutamate receptors, both metabotropic (mGluR5) and ionotropic (AMPA and NMDA).9 The synthesis, degradation, and transport proteins of g-aminobutyric acid (GABA) and GABA receptors are also reduced.10 It is not known exactly how these changes in neurotransmitter systems affect the morphology of dendrites and spines in neurons, but it is suspected that they are related. The role of the FMRP protein in glial cells is less known, but it is known that in FXS, the FMRP protein regulates the translation of mGluR5 into astrocytes11 and the production of myelin in oligodendrocytes.12 During prenatal development, radial glial cells contain FMRP, which is involved in the active transport of mRNA along the glial fiber.13 A change in any of these mechanisms can contribute to the development of cognitive disorders in patients with SXF.
Expanded CGG repetitions are common, intermediate, premutation, and complete mutation alleles. The common alleles in the general population generally contain 6 to 40 repetitions of CGG that are stable and generally do not expand in the transmission from the parents to the offspring. Intermediate alleles containing 41-60 CGG repeats have variable expansion risks, while premutation alleles (i.e., 55-199 CGG repeats) are generally not methylated.14 Repetition can become unstable after maternal transmission, which usually results in the expansion of repetition in the next generation. When repetition expands and ranges between 55 and 200, individuals are considered carriers of premutation. In patients with FXS, the repetition of CGG has expanded to more than 200 units.15
The mechanism underlying the increase in transcriptional activity of the alleles of the premutation range is unknown. However, a recent study reported the differential use of transcriptional initiation sites and polyadenylation sites in FMR1 premutation alleles, leading to different expressions in expanded premutation alleles compared to normal alleles.16
Primary Ovarian Insufficiency (Poi) in Patients with Fmr1 Gene Mutation
Only 1% of women experience menopause before the age of 40, called POI. This is the “final stage” of continuous ovarian dysfunction, and despite its clinical importance, the etiology of the POI is often not identified. Women with premutation are at risk of premature ovarian insufficiency (primary ovarian insufficiency associated with fragile X; FXPOI). It has been shown that women with a certain premutation through families with FXS have a POI rate of up to 23% and, as a group, experience a previous menopause in approximately 5 years.17 Currently, there is no consensus on estimating the absolute risk of POI when a woman has normal or high intermediate repetition alleles. Several studies have been estimated at between 15% and 27% in premutation carriers, compared to a background risk of 1%.18
Regardless of the cause, in women with established POI, the opportunity to preserve fertility is lost due to the loss of most of the reproductive material. In this case, recent guidelines still report oocyte donation as the only realistic option for pregnancy.19
This type of treatment must also be cryopreserved to preserve a couple’s or a woman’s fertility. If premature ovarian insufficiency is predicted long before the onset of early menopause, patients at risk of this condition could benefit from the preservation of fertility due to cryopreservation of reproductive material.20
A pre-implantation genetic diagnosis should be suggested to prevent the birth of offspring affected by the complete FMR1 mutation. In this case, PGT-M is the preferred method for selecting and cryopreserving suitable embryos or using them in IVF programs.20
Clinical Presentation of Patients Affected with Complete Mutation of The FMR1 Gene
Patients affected by the complete mutation of the FMR1 gene have special phenotypic characteristics, including an elongated face, large and prominent ears, joint hypermobility, and macroorchidism.21
More than 90% of affected children have developmental delays, and approximately 50-60% are diagnosed with Autism Spectrum Disorder (ASD).22 Throughout their lives, both men and women have behavioral alterations commonly associated with the syndrome, usually beginning during childhood: anxiety and attention and hyperactivity disorder (ADHD) are the most prevalent. However, compulsive disorders such as hyperphagia and aggressiveness are also common. Some characteristics reported in patients with a complete mutation of the FMR1 gene are summarized in TABLE 3.
Use Of Androgens in Patients with Low Response Undergoing In Vitro Fertilization
The poor ovarian response results from inadequate ovarian stimulation, generally defined by a low number of recovered oocytes or a low number of developing follicles and a low concentration of estradiol in a previous or functioning IVF cycle.23
It has been suggested that the accumulation of androgens in the microenvironment of the ovary plays a fundamental role in early follicular development and the proliferation of granulosa cells.24 Excess androgens have been shown to stimulate the early stages of follicular growth25 and increase the number of preantral and antral follicles.26 In addition, the increase in the intraovarian concentration of androgens seems to increase the expression of the follicle-stimulating hormone (FSH) receptor in the granulosa cells27 and, therefore, potentially lead to a greater response of the ovaries to FSH.28
Low ovarian reserve is considered one of the most frequent causes of infertility and is considered one of the main challenges in reproductive medicine. Numerous studies have suggested that androgens (dehydroepiandrosterone and testosterone) play an important role in follicular development by increasing the number of oocytes, thus increasing the pregnancy rate. Testosterone is a sex steroid hormone that originates from cholesterol and is considered a precursor of estradiol biosynthesis.29
Previous treatment with transdermal testosterone has been suggested as a safe and effective way to increase the intraovarian concentration of androgens.30
Recently published randomized controlled trials (RCTs) have evaluated transdermal testosterone31 or the pre-treatment of DHEA.32 In people with poor response who undergo ovarian stimulation for IVF, with inconclusive results and others with notable benefits in a number of oocytes, embryo development, and pregnancy rates.
Conclusions
FMR1 premutation is associated with the risk of reduced ovarian function and premature ovarian failure with early loss of fertility in 20% of women carriers due to the reduced number of follicles in the ovaries.
Patients with POI have lower levels of E2 and lower levels of AMH and undergo menopause, on average, 5 years earlier than non-carrier women. Suppose an early diagnosis of a genetic alteration related to POI is made. In that case, precise genetic advice is required for the patient and her family, as well as an evaluation for the preservation of fertility, as soon as possible.
It is necessary to consider specific clinical and ethical issues regarding the possible association with syndromic clinical conditions, as well as the different mechanisms that led to a poor ovarian response, which increases the complexity of choosing the most appropriate fertility preservation techniques.
In this case, the patient did not want to carry out a pre-implantation genetic study due to the low risk of aneuploidy according to age; she does not accept PGTm either. It is considered to make a fresh transfer since its hormonal levels allow an adequate endometrial thickness.
According to the limited available evidence, transdermal testosterone pretreatment seems to increase pregnancy and the rates of live births in people considered as low responders who undergo ovarian stimulation for IVF. We consider that having been with greater exposure to transdermal testosterone before and during the second controlled ovarian stimulation can improve the number of mature oocytes obtained in the second cycle and thus increase the chances of having embryos developed for embryo transfer. Although several studies suggest the use of testosterone as a safe treatment to increase the number of mature oocytes in fertility treatments, more studies are required to validate the effectiveness and safety of this treatment.
Authors’ Contribution - CRediT
Conceptualization: Fernando Mancilla Hernández (Lead). Resources: Fernando Mancilla Hernández (Lead). Writing – review & editing: Fernando Mancilla Hernández (Lead). Data curation: Jorge L. Lezama Ruvalcaba (Lead). Project administration: Jorge L. Lezama Ruvalcaba (Lead). Supervision: Jorge L. Lezama Ruvalcaba (Lead). Writing – original draft: Jorge L. Lezama Ruvalcaba (Lead). Formal Analysis: Ricardo Rodríguez Calderón (Lead). Software: Ricardo Rodríguez Calderón (Lead). Funding acquisition: Carlos G. Salazar López-Ortiz (Lead). Validation: Carlos G. Salazar López-Ortiz (Lead). Methodology: Paola R. Becerril Rodríguez (Lead). Investigation: Julio C. Rodríguez Verduzco (Lead). Visualization: Julio C. Rodríguez Verduzco (Lead).
Competing of Interest – COPE
No competing interests were disclosed.
Informed Consent Statement
All authors and institutions have confirmed this manuscript for publication.
Data Availability Statement
All are available upon reasonable request.