Introduction
Over the past forty years since its inception, advances in assisted reproductive technology (ART) have led to a dramatic improvement in the success rates of fertility treatments. Frozen-thawed embryo transfer (FET) has been widely used in in vitro fertilization (IVF), due to its capacity to improve fertility and pregnancy outcomes, prevent ovarian hyperstimulation syndrome, and enable single embryo transfer.1 FET & blastocysts have been more frequently carried out and have demonstrated to reduce the number of multiple pregnancies while increasing the cumulative pregnancy rates for individual patients.2 Fresh embryo transfer performance has shown to decrease from 85.5% in 2010 to 79.8% in 2011, whereas FET increased concurrently from 29.7% in 2010 to 31.3% in 2011.2 Frozen embryo transfer not only enhances neonatal outcomes but also seems to reduce the risk of an ectopic pregnancy.3
As assisted reproductive technologies have advanced over the past four decades, fertility treatment success rates have increased dramatically making it possible for IVF to examine follicle growth, fertilization, and embryo development more closely, although peri-implantation events are still not widely available. Endometrial receptivity, often known as the “window of implantation,” refers to the complex and precise communication between the embryo and endometrium that must be in complete synchronization during a specific time frame for successful embryo implantation.4 However, there are still unresolved issues about the best way to prepare the endometrium.5
The endometrium must be prepared for the optimal implantation for FET to function. The two most popular methods for endometrial preparation are the natural cycle (NC) and hormone replacement therapy (HRT) cycles. To prepare the endometrium and avoid excessive hormonal exposure and the negative effects that come with it, a dominant follicle that produces estradiol develops spontaneously in NC.
NC can be carried out as a genuine natural cycle or with hCG-triggered ovulation, and it is particularly advantageous for women who have regular menstrual cycles. On the other hand, HRT uses exogenous progesterone and estrogen to prepare the endometrium, providing patients and clinicians with logistical advantages like predictability and flexibility.6
Although both NC and HRT are widely used across different IVF centres in the world, it is still unknown what would be the best endometrial preparation method. Recent systematic reviews and meta-analyses, including those by Pan et al.7 and Liu et al.,8 continue to highlight the lack of definitive evidence favoring one endometrial preparation method over another for FET cycles. Equally, pregnancy outcomes using the two approaches have not been found to differ significantly in systematic reviews or meta-analyses.9,10 However, because of the lack of the corpus luteum, HRT cycles have been linked to an increased risk of maternal problems, including hypertensive disorders during pregnancy.11
There is also conflicting information about clinical outcomes such as miscarriage rates and live birth rates (LBR) between NC and HRT cycles. A large retrospective analysis of 14421 cycles demonstrated significantly higher early pregnancy loss rate with HRT cycle in comparison with NC (36.5% vs 25.7% vs 23.6%, respectively, P < 0.005) whilst the live birth rate was significantly lower for HRT compared with NC.12 While some research indicates that HRT produces better results,13,14 other research contradicts this and claims that NC yields superior outcomes.15,16
Few randomized controlled trials (RCTs) have been conducted to address this problem; however, methodological challenges and insufficient sample sizes have prevented definitive results.17,18 Given the conflicting findings and the critical role endometrial preparation plays in FET success, more research is required. This study aims to examine clinical pregnancy and live birth rates (LBR) between NC and HRT cycles while taking important demographic variables like age and BMI into account. This retrospective study aims to offer solid evidence for CPR & LBR to support clinical judgement in endometrial preparation techniques by concentrating on two primary protocols used in FET cycles while considering several demographic variables, including age and BMI, use of euploid, vitrified-warmed blastocyst transfers.
Materials and Methods
Study methodology
This retrospective study was carried out over the course of 12 months duration, from January to December 2022 at the Fakih Fertility Centre in Abu Dhabi, United Arab Emirates. This investigation employed a retrospective design, allowing us to analyze a substantial cohort of patients (n= 379) who underwent frozen embryo transfers (FET) via either Hormone Replacement Therapy (HRT) (n=324) and Natural Cycle (NC) (n=55) protocols where euploid blastocyst were included in the analysis.
The retrospective nature of the study provides several advantages, including the ability to access existing data from medical records, which facilitates the inclusion of a larger and more diverse patient population within a shorter timeframe compared to prospective studies. Furthermore, retrospective studies enable the examination of real-world clinical practices and outcomes, thereby enhancing the generalizability of the findings.
However, it is important to acknowledge the limitations inherent in this design. Retrospective studies are subject to biases, such as selection bias and information bias, which can arise from reliance on previously collected data that may not have been initially intended for research purposes. This retrospectively derived data may also face challenges related to completeness and accuracy, impacting the reliability of some outcomes. Nonetheless, by carefully selecting and reviewing cases and employing rigorous statistical analyses, this study aims to mitigate these limitations and yield valuable insights into the comparative effectiveness of HRT and NC protocols in frozen embryo transfers.
Patients’ demographic criterion for inclusion and exclusion:
Patients were considered eligible if they met the following criteria: [1] women who had previous IVF cycles with embryo cryopreservation, [2] 20–40 years of age, [3] first cycle of FET, and [4] regular menstrual cycles (25–35 days). The exclusion criteria were [1] endometriosis, [2] no preimplantation genetic testing cycles [3] uterine pathology, or [5] cycles aborted because embryo thaw survival was unsuccessful were the exclusion criteria.
Definition of Clinical Outcomes
For the clinical outcomes, we employed the 2017 consensus definitions provided by the American Society for Reproductive Medicine (ASRM).19 A clinical pregnancy was defined as one that was identified by clear clinical indications of pregnancy or by the ultrasonographic visualization of one or more gestational sacs. A delivery that occurs after 22 weeks but before 37 full weeks of gestation is considered preterm. The number of gestational sacs seen divided by the number of transplanted embryos was the definition of the implantation rate. The delivery of at least one live infant after 22 weeks of gestation was referred to as a live birth. The term “live-birth rate” refers to the number of live births (at least one per woman) following embryo transfer.
Participants
Women undergoing FET cycles were retrospectively analyzed and categorized into the NC or HRT group according to physician guidance. The study included patients across different age groups, BMI and AMH levels categories as shown in table 1. The mean age of the patient recruited were 33.71 years, BMI 27.37 and AMH levels of 4.44 ng/ml.
Treatment protocol
HRT Protocol: Patients received a standardized regimen involving estradiol and progesterone
Method
In HRT stimulated cycle, the patients undertook urine human chorionic gonadotrophins (hCG) test and transvaginal scan on the second day of menstruation first. Baseline hormones, serum FSH, LH, Oestradiol and progesterone was undertaken on the same day. If level optimum, then oral estradiol tablets (4–6 mg/d, Bayer, Leverkusen Germany) were given according to the endometrium thickness of the previous fresh cycle. The estradiol tablets were given in escalated doses to achieve optimum endometrial thickness. Vaginal ultrasound was performed 10 days later to measure the endometrium thickness. Adequate endometrial preparation was defined as an endometrial thickness of at least 7 mm with trilaminar appearance.20 Once the endometrium was adequately prepared, serum progesterone levels were measured after the endometrial assessment. Once the endometrium thickness reached 7 mm or more as assessed by transvaginal scan, Progesterone supplementation was initiated and was administered orally (Dydrogesterone 10 mg twice daily along with micronized progesterone vaginal suppositories 400 mg twice daily). Other than the above they also received Intramuscular progesterone in oil every three days. A maximum of two blastocysts were transferred after 5 days of progesterone supplementation.
All patients subsequently received & continued our standard luteal support that includes, oral oestradiol tablets in escalated doses, transvaginal progesterone, Intramuscular progesterone in oil every three days, 20 mg of oral dydrogesterone. The transfer was cancelled if the serum progesterone value was more than 1.5 ng/ml. Blastocyst transfer was scheduled on D6 if the day commencing progesterone was D0 and a maximum of two Euploid embryos were transferred 5 days after starting the luteal support under transabdominal ultrasound guidance as described before.21 Serum beta human chorionic gonadotropin (ß -hCG) levels were measured 10 days after embryo transfer to confirm pregnancy outcomes. If serum ß-hCG was positive, luteal support was continued and an ultrasound examination was carried out 2 weeks later to assess clinical pregnancy for positive fetal heart, miscarriage, and ongoing viable pregnancy. The dose of estrogen was stopped in case viable pregnancy was confirmed by ultrasound whilst the rest of luteal support medication was continued till 12 weeks of gestation.
In the Natural Protocol (NC), patients followed their natural menstrual cycle with minimal medical intervention termed as modified NC. Women in the modified NC group underwent transvaginal ultrasound from the start of menstrual cycle similar to the HRT cycle. Follicular growth was monitored through transvaginal ultrasound and serum luteinizing hormone (LH). When LH >20 IU/L, follicular study was continued till a dominant follicle of 16 or 18 mm was identified with a triple line endometrium 7mm or more. Recombinant hCG (Ovitelle) was given to trigger oocytes ovulation and embryo transfer was planned on hCG+7 days. When the ovulation was confirmed by transvaginal ultrasound, 400 mg of vaginal micronized progesterone was initiated two times a day and continued till the day of blastocyst transfer. Thereafter, progesterone support was continued until 12 weeks of gestation.
Data Collection and Analysis
Data were collected on demographic variables (age, BMI), clinical parameters (AMH levels), and cycle characteristics (number of embryos transferred). Outcomes measured included clinical pregnancy rates (CPR).
Statistical Analysis
Qualitative attributes are described by numbers and percentages. The proportions, CPR, and LBR were compared using chi-squared tests. Continuous variables were compared using ANOVA. In univariate or multivariable analyses, continuous variables—also referred to as clinically relevant classes—were included. Using logistic regression analysis, factors associated with age BMI and the likelihood of early pregnancy loss were identified. Variables were analysed according to their relevance or significance in the numerous comparison studies that were conducted. The variables that were included in the multivariable model were those that had a P of 0.20 in univariate analysis and were associated with the likelihood of early pregnancy loss. The significance threshold was established using a P-value of 0.05. For statistical analysis, SAS software version 9.4 was utilized.
Results
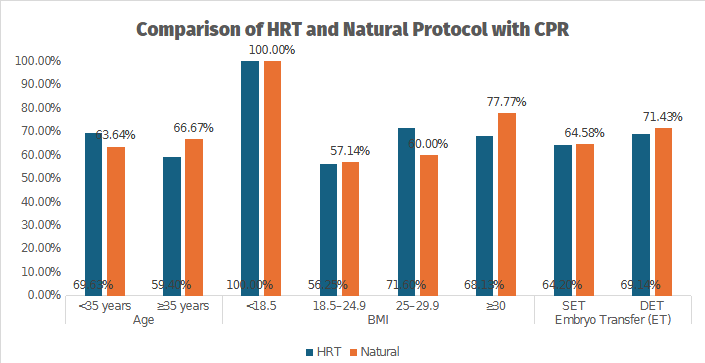
Demographics and baseline characteristics the mean age of participants was 33.71 ± 5.63 years, and the mean BMI was 27.37 ± 5.22 (Table 1). The average number of embryos transferred was 1.23 ± 0.42. The results revealed no significant difference in the effectiveness of HRT and NC with CPR standing at 65.43% for HRT and comparable outcomes of 65.45% for NC (Table 2, Figure 1). CPR calculated as the proportion of gestational sacs observed on ultrasonography to the number of transferred embryos, for the two treatment groups is presented in Table 2. When compared with the single embryo transfer, CPR was comparable in both groups. However, in patients with double embryo transfer, there was a subtle difference where the NC group exhibited a marginally higher success rate (71.43%) compared to HRT (69.14%) (Table 2, Figure 1). Stratification by age indicated nuanced differences where patients under 35 years in the HRT group exhibited a marginally higher success rate (69.63%) compared to NC (63.64%). Conversely, in patients above 35 years, the NC slightly outperformed HRT with CPRs of 66.67% and 59.40% respectively, not reaching statistical significance. In terms of BMI, the HRT cycle was most effective in patients between 25 and 29.9, while the NC showed the highest effectiveness in patients with a BMI above 30 with a significant p-value of 0.042 (Table 2, Figure 1).
__bmi_categories_(_18.5__18.524.9__.png)
With single embryo transfer, CPRs were comparable between the HRT and NC groups (Table 2, Figure 1). For double embryo transfer, the NC protocol showed a marginally higher success rate (71.43%) compared to HRT (69.14%). Among patients under 35 years, the HRT group exhibited a slightly higher CPR (69.63%) compared to NC (63.64%). In patients over 35 years, the NC protocol demonstrated a higher CPR (66.67%) than HRT (59.40%), though this difference was not statistically significant.
In terms of BMI, the HRT protocol was most effective in patients with a BMI between 25–29.9, achieving a CPR of 71.60%. Meanwhile, the NC protocol demonstrated the highest effectiveness in patients with a BMI ≥30, with a CPR of 77.77%, achieving statistical significance (p = 0.042).
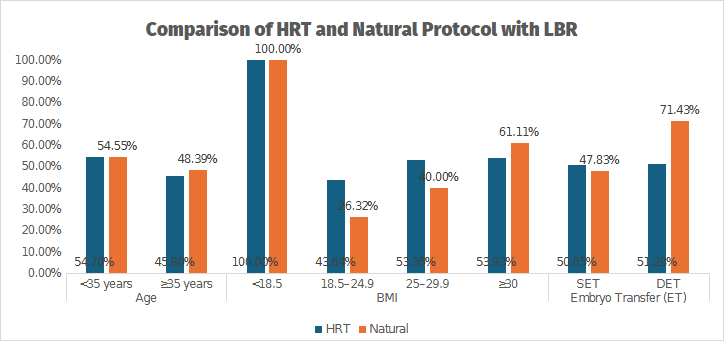
In terms of live birth, a total of 365 patients’ data was analyzed. The mean age of patients was 33.24±5.63 with a mean BMI of 27.38± 5.23 and these patients AMH was 4.47±4.23 (Table 4). The LBR was similar between the two groups with no significant difference seen in the effectiveness of HRT (50.96%) and NC (49.06%) (Table 3, Figure 2). Stratification by age indicated nuanced differences where patients more than 35 years in the NC group exhibited a marginally higher success rate (48.39%) compared to HRT (45.80%) not reaching statistical significance. Whilst, in patients less than 35 years, both groups had comparable outcomes of 55.70% (HRT) & 54.55% (NC). In terms of BMI, the HRT cycle was most effective in patients between 25 and 29.9, while the NC showed the highest effectiveness (61.11%) in patients with a BMI above 30 although not reaching statistical significance with a significant p-value of 0.212. When compared with the single embryo transfer, LBR was comparable in both groups. However, in patients with double embryo transfer, there was a difference observed where the NC group exhibited a marginally higher success rate (71.43%) compared to HRT (51.28%) but not reaching statistical significance.
__bm.png)
The overall LBR was comparable between HRT (50.96%) and NC (49.06%) protocols. patients aged >35 years, the NC group exhibited a slightly higher LBR (48.39%) compared to HRT (45.80%), though this difference was not statistically significant. Among patients <35 years, outcomes were similar in both groups (HRT: 55.70%, NC: 54.55%).
In terms of BMI, the HRT protocol was most effective for patients with BMI 25–29.9, while the NC protocol showed the highest effectiveness (61.11%) in patients with BMI ≥30, although this difference did not reach statistical significance (p = 0.212).
For SET, LBR was comparable between the two groups. However, with DET, the NC group demonstrated a marginally higher success rate (71.43%) compared to HRT (51.28%), though the difference was not statistically significant.
Discussion
This retrospective cohort study compared live birth rates (LBR) between natural cycle (NC) and hormone replacement therapy (HRT) protocols in frozen embryo transfer (FET) cycles, considering variables such as patient age, BMI, number of embryos and embryo transfer type. The findings highlight that the overall LBR was comparable between the two protocols. For patients aged over 35 years, NC exhibited a slightly higher LBR, though this difference was not statistically significant. As BMI also played a role, with HRT being most effective for patients with a BMI of 25–29.9, while NC showed higher effectiveness for patients with a BMI ≥30. This is in line with other recent studies, including Pan et al.7 and Vinsonneau et al.,12 that showed that while hormone therapy enables precise scheduling of embryo transfer, they suggest that NC protocols may offer comparable or slightly superior outcomes in specific subgroups, such as patients with higher BMI.
Similarly, double embryo transfer (DET) outcomes favored NC, suggesting a marginal benefit with this protocol. However, the most recently published Cochrane review concluded that to date, there is no evidence to support the use of 1 preparation method above another when considering implantation rates and/or live birth rates (LBRs). But the use of preimplantation genetic testing for aneuploidy (PGT-A) in our study provided robust data by controlling for embryonic factors, allowing a clearer evaluation of endometrial preparation. These findings align with several published studies, although the literature presents conflicting evidence. For instance, studies by Kim et al. showed no significant differences between HRT and NC outcomes. On the contrary, studies by other researchers16,22,23 suggested better clinical outcomes with NC, supporting the findings consistent with the present study.
The use of NC protocol for endometrial preparation in FET cycle is thought to be more natural and safer method than exposing the patients to the risk of exogenous hormones. Therefore, patients can be counselled with confidence about no risk of side effects or complications in relation to hormone therapy. Moreover, with the NC protocol will have reduced costs implications to the patients. Other than that, the body’s natural hormones regulate the cycle, which might create a more favourable environment for embryo implantation. It has been shown that the corpus luteum that forms in the NC, clearly plays a significant part in the cardiovascular adaptation of the mother to pregnancy.24 In addition to that the corpus luteum secretes a variety of vasoactive substances, including renin, relaxin, oxytocin, progesterone, aldosterone, and vascular endothelial growth factor.25
Physiologically, NC cycles utilize the body’s natural hormonal regulation, minimizing risks associated with exogenous hormones. The corpus luteum, formed during NC, plays a critical role in maternal cardiovascular adaptation and the secretion of vasoactive substances such as relaxin, oxytocin, and progesterone.24,26 This could mediate improved maternal circulatory function hence having beneficial impact of NC on clinical pregnancy outcomes by more closely mimicking physiological conditions and these factors might contribute to a more favorable environment for embryo implantation. The cost-effectiveness and lack of hormone-related side effects of NC procedures further increase its allure.27 However, NC’s unpredictable ovulation can make managing cycles more difficult, necessitating regular monitoring and raising the possibility of cycle cancellations. Because of these difficulties, HRT is frequently a desirable substitute for both patients and doctors.
Convenient scheduling of embryo transfers is made possible by HRT’s consistent scheduling and lower monitoring needs. However, hormone therapy may not be appropriate for all people and might cause adverse effects like bloating, headaches, and mood swings. In addition, the adverse effects of exposure to exogenous hormones may lead to a higher risk of thromboembolic events and could damage placentation, which may in turn cause miscarriage.28 The higher costs associated with medications and frequent visits also pose challenges.
Studies by Li et al. and Vinsonneau et al.12,29 showed comparable clinical pregnancy rates between HRT and NC despite these trade-offs, supporting the results of this investigation. Additionally, others have30,31 found that euploid blastocyst transfers had increased LBR in NC, which supports the findings of the current study.
Another important element affecting results is the timing of the embryo transfer. Careful planning is necessary due to the implantation window’s unpredictability. Although this study considered day 0 as the beginning of progesterone administration and scheduled blastocyst transfers for HRT cycles on day 6, other investigations have taken a different tack. These differences, along with variations in patient demographics, might explain discrepancies across studies. The Middle Eastern population in this study adds another layer of distinction, emphasizing the need for tailored protocols based on regional and individual characteristics.
The study’s strengths lie in its use of PGT-A to standardize embryo quality and its comprehensive analysis of variables such as age, BMI, and ovarian reserve. The real-world data enhances the findings’ applicability, particularly as FET cycles continue to rise.
Limitations
This study has several limitations. First, its retrospective design introduces inherent biases, including selection bias and information bias, which may affect the interpretation of results. Additionally, the non-randomized grouping of patients into HRT and NC protocols leaves room for physician bias in protocol selection, potentially influencing outcomes.
Second, the findings may lack external validity due to the single-centre design, which limits generalizability to broader populations. The demographic and clinical characteristics specific to this study’s patient cohort may not reflect those of other populations.
Third, the unequal sample sizes between HRT and NC groups may have impacted statistical power, limiting the detection of significant differences in outcomes. Furthermore, confounding variables such as lifestyle factors, male infertility, and genetic differences were not accounted for, which may influence the observed results.
Future research should address these limitations by employing randomized controlled trials (RCTs) to minimize bias and improve generalizability. Larger multicentre studies with diverse patient populations are recommended to validate these findings and ensure broader applicability. Incorporating additional confounding factors into analyses would further refine protocol comparisons and strengthen clinical recommendations.
Conclusions
This study highlights the importance of tailoring fertility treatments to individual patient profiles, emphasizing the role of BMI and age in protocol selection. Patients with BMI ≥30 may benefit more from NC protocols, particularly when opting for double embryo transfers. Given the comparable success rates observed between HRT and NC, clinicians can adopt a personalized approach that factors in patient demographics and preferences while minimizing unnecessary interventions.
To further guide clinical decision-making, we propose that BMI-specific guidelines be developed to optimize protocol selection and improve outcomes. For patients with higher BMI, NC may provide a safer, cost-effective alternative with reduced hormone exposure. However, HRT remains a viable option for patients requiring cycle predictability and convenience.
Future randomized controlled trials are necessary to validate these findings and refine treatment strategies, ensuring patients receive the most effective care tailored to their needs.
Funding Statement
There has been no funding received for this study.
Competing Interest
None
Submission declaration & Declaration of interest
The manuscript has never been published before. There are no other publications considering it.
The author(s) declares no conflict of interest and have no relevant affiliations or financial involvement with any organization or entity with a financial interest. This includes employment, consultancies, honoraria, expert testimony, grants or royalties.
Ethics approval and consent to participate
This study was conducted in strict adherence to ethical principles and guidelines. All efforts were made to safeguard the confidentiality and privacy of their personal information throughout the study.
Data Availability Statement
The data supporting the findings of this study are stored in software called Meditex, which is designed specifically for In-Vitro Fertilization (IVF) clinics. Meditex serves as a tool for managing and documenting patient data within Assisted Reproduction organizations. However, it’s important to note that there are restrictions on accessing this data due to licensing agreements for this study. Therefore, the data cannot be accessed publicly. Nevertheless, the authors of the study are willing to provide access to the data upon request.
Author’s contributions
All the authors contributed equally to this article.
Acknowledgement
The authors thank Ms. Sahana Chandrappa Biostatistician and Ms. Gladies (Academic program coordinator) for their support in this study.