Introduction
FP has emerged as a critical component of comprehensive cancer care, particularly for patients of reproductive age facing gonadotoxic treatments. The American Society of Clinical Oncology (ASCO) has established clear guidelines recommending that all patients of reproductive age receive counseling about fertility risks and preservation options before initiating cancer therapy.1 However, despite guideline support, patients with hematologic cancers are 20–30% less likely to undergo fertility preservation compared to those with solid tumors, with reported uptake rates as low as 9% versus 40%, respectively2,3 (Table 1).
Hematologic malignancies affect approximately 174,000 individuals annually in the United States, with nearly 40% diagnosed during their reproductive years (ages 15-45). Unlike solid tumors where fertility preservation can often be planned around surgical schedules, blood cancers frequently require immediate therapeutic intervention, compressing the typical 2–4-week fertility preservation window to days or hours. This urgency, combined with disease-specific factors such as thrombocytopenia, coagulopathy, and the risk of malignant cell contamination in reproductive tissues, creates implementation challenges not adequately addressed in general oncofertility guidelines.5
Recent global data confirm that patients with hematologic malignancies experience 20-30% lower uptake and utilization of fertility preservation compared to those with solid tumors, despite evidence showing meaningful reproductive success rates (live births: 4.6-41%) when preservation is pursued.2,3 The 2025 ASCO guideline update endorses embryo, oocyte, and ovarian tissue cryopreservation (OTC) for eligible patients and introduces in vitro maturation (IVM) as a promising option when urgent treatment precludes standard ovarian stimulation.1 Although ovarian reserve, as measured by anti-Müllerian hormone (AMH), is often diminished in this population, studies indicate that appropriately timed stimulation protocols can yield mature oocyte numbers comparable to healthy controls.6 These findings highlight the feasibility of FP in hematologic oncology, even under time constraints, when disease-specific strategies are implemented.2,6
While provider-reported counseling rates have improved from historical levels below 50 % to 75 %–95 % in specialized centers, significant variability persists across practice settings. A global survey of 266 hematopoietic cell-transplant specialists revealed that although 91 % considered fertility preservation important, only 44 % routinely referred patients for consultation, with treatment urgency cited as the primary barrier in 83 % of cases.4 This implementation gap disproportionately affects hematologic-oncology patients, who face compressed timelines that leave minimal opportunity for standard preservation protocols. Prior expert reviews have emphasized the importance of early, tailored discussions to support reproductive autonomy in this population.7–9 However, these reviews have largely extrapolated from solid-tumor data or provided general recommendations without addressing the specific clinical complexities inherent to hematologic malignancies. These include the need for immediate treatment initiation, heightened contamination risk with ovarian tissue uses, and a markedly limited window, sometimes mere days, for implementing preservation strategies. As a result, existing guidelines and expert reviews frequently lack urgency-specific protocols tailored to blood cancers, leaving clinicians without clear, actionable pathways in these high-stakes scenarios.
Research Rationale and Objectives
This review addresses a critical gap in oncofertility practice by providing one of the first comprehensive, disease-specific clinical frameworks for fertility preservation in hematologic malignancies. Our analysis addresses five key research questions:
-
What are the current patterns of fertility preservation counseling, utilization, and outcomes specifically in hematologic malignancy patients?
-
How can existing gonadotoxicity risk assessments be refined for disease-specific decision-making in blood cancers?
-
Which emerging preservation techniques are most suitable for urgent implementation in hematologic oncology?
-
What fertility risks are associated with novel hematologic therapies, and how should these inform counseling?
-
What ethical and equity considerations are unique to fertility preservation in this population?
Unlike existing general reviews that primarily extrapolate from solid tumor data, we synthesize evidence specifically addressing the unique challenges of blood cancers: treatment timelines compressed to days rather than weeks, disease-specific contamination risks requiring molecular screening, and emerging therapies with uncertain fertility impact. Our analysis translates broad guideline recommendations into immediately implementable, risk-stratified protocols that acknowledge the distinct decision-making pressures faced by hematologic patients and their care teams. We provide evidence-graded gonadotoxicity assessments, disease-specific preservation algorithms, and practical tools for time-sensitive fertility counseling that can be integrated into urgent oncology workflows.
Materials and Methods
This narrative review synthesizes current literature on fertility preservation in patients with hematologic malignancies, with a focus on clinical outcomes, implementation practices, and ethical considerations. A targeted literature search was conducted using PubMed and Embase for peer-reviewed articles published between 2010 and 2025.
Search Strategy
Given the distinct clinical challenges of hematologic malignancies, including treatment urgency, malignant cell contamination risks, and evolving therapeutic landscapes, this review prioritizes synthesis of actionable, disease-specific guidance over general fertility preservation principles. We emphasize practical implementation strategies, contemporary outcome data specific to hematologic patients, and evidence gaps requiring specialized counseling approaches.
Inclusion and Exclusion Criteria
Inclusion criteria were English-language studies involving human subjects that addressed fertility preservation in the context of hematologic cancers, including leukemia, lymphoma, and multiple myeloma. Search terms included combinations of “fertility preservation,” “hematologic malignancies,” “oncofertility,” “cryopreservation,” and disease-specific terms (including “leukemia,” “lymphoma,” “multiple myeloma,” “bone marrow transplant,” and “hematopoietic stem cell transplant”).
Eligible sources included randomized controlled trials, observational studies, cohort studies, systematic reviews, meta-analyses, clinical guidelines, and relevant ethical position papers. Exclusion criteria included animal studies, case reports with fewer than five patients, and non-peer-reviewed commentaries unless they provided guideline-level insights from major professional organizations.
Study Selection and Data Extraction
Priority was given to high-quality publications from leading oncology, reproductive medicine, and bioethics journals, as well as updates from authoritative bodies such as the American Society of Clinical Oncology (ASCO), the American Society for Reproductive Medicine (ASRM), and the National Comprehensive Cancer Network (NCCN). Studies were selected based on relevance to hematologic malignancies, clinical impact, and evidence quality, with priority given to systematic reviews and guidelines. Studies were categorized by evidence level and clinical relevance to hematologic oncology practice.
Synthesis Approach
This review aims to: (1) synthesize current evidence on fertility preservation counseling, utilization, and outcomes specific to hematologic malignancies; (2) provide disease-stratified risk assessment tools for preservation decision-making; (3) evaluate emerging preservation techniques suitable for urgent implementation; (4) analyze the fertility impact of novel hematologic therapies; and (5) address ethical and equity considerations unique to this population. Our goal is to transform general fertility preservation principles into specialized, immediately actionable guidance for hematologic oncology practice.
Quality Assessment
Evidence quality was assessed using established frameworks, with preference given to systematic reviews, randomized controlled trials, and large cohort studies. For emerging therapies with limited human data, preclinical studies and expert consensus statements were included with appropriate caveats regarding evidence limitations.
As this is a narrative review, the selection and synthesis of included studies may be influenced by interpretation bias, and some relevant publications may not have been captured despite efforts to ensure comprehensive coverage. The absence of a systematic screening protocol may also limit reproducibility.
Manuscript Preparation
Artificial intelligence tools were used to support language refinement, stylistic consistency, and reference formatting throughout the manuscript. All content was authored and reviewed by the manuscript authors to ensure scientific accuracy and integrity. The synthesis follows established guidelines for narrative reviews while maintaining focus on clinical applicability and immediate implementation potential.
Results and Discussion
The following synthesis is organized around the key implementation challenges that distinguish fertility preservation in hematologic malignancies from other cancer types. Rather than recapitulating general oncofertility principles, we focus on specialized strategies for time-sensitive decision-making, disease-specific risk stratification, and novel therapy considerations that define contemporary hematologic oncology practice.
Counseling and Utilization Disparities
Provider-Reported Implementation Gaps
Despite established international guidelines, fertility preservation counseling and utilization in patients with hematologic malignancies remain inconsistent and frequently inadequate. Compared to solid tumor patients, those with hematologic cancers are less likely to receive timely counseling or undergo fertility preservation procedures.8,10,11 A global survey of 266 hematopoietic cell transplant specialists across 52 countries revealed a significant practice gap: while 91% considered fertility preservation important, only 44% routinely referred patients for consultation.4
Patient-Reported Experiences
This provider-patient disconnect is reflected in patient-reported experiences across cancer types. The Adolescent and Young Adult (AYA) HOPE Study found that only 74% of women with cancer were informed about fertility risks, with significantly lower rates among minorities, less-educated, or uninsured patients.12 Patients frequently report that fertility discussions, when they occur, are delayed, inadequate, or delivered during emotionally overwhelming diagnosis visits.13
Primary Implementation Barriers
Treatment urgency emerged as the dominant barrier in hematologic oncology, cited by 83% of providers, followed by lack of access to fertility specialists (53%) and financial limitations (50%).4 Regional disparities and variation in practice settings further compound these barriers, highlighting a persistent disconnect between physician awareness and clinical implementation in a field where treatment timelines are compressed and preservation opportunities are limited.
Barriers to Counseling and Utilization
Several factors contribute to reduced rates of FP among patients with hematologic malignancies:
-
Urgency of treatment: Hematologic cancers often require immediate initiation of chemotherapy or conditioning regimens, leaving insufficient time for FP procedures involving ovarian stimulation or tissue retrieval.7,8
-
Limited preservation options for pediatric and prepubertal patients: Standard cryopreservation techniques are not feasible in these populations, and alternatives such as ovarian or testicular tissue preservation remain investigational or limited in availability.14
-
Risk of malignant contamination: In diseases such as leukemia, preserved ovarian tissue may harbor malignant cells, raising concerns about reintroduction of disease upon transplantation.15,16
-
Provider and institutional constraints: Many oncology clinicians report inadequate training or discomfort discussing FP, compounded by the lack of streamlined referral pathways.11
-
Sociodemographic inequities: Patients from minority backgrounds, lower socioeconomic status, or private care settings, as well as older individuals and males, are less likely to receive fertility counseling or be referred to preservation services.10,17
-
Patient perspectives illuminate the real-world impact of these barriers. Qualitative studies reveal that the threat of infertility significantly affects quality of life, with patients experiencing anxiety, grief, and concerns about future relationships.13 The compressed timelines characteristic of hematologic malignancies exacerbate this distress, as patients report feeling ‘rushed into decisions’ about fertility preservation while simultaneously processing their cancer diagnosis.18 Men generally find sperm cryopreservation straightforward, while women describe the complexity of oocyte/embryo preservation as overwhelming when combined with urgent treatment needs.
Facilitators of Counseling and Institutional Strategies
Despite these challenges, several institutional and clinical strategies have been shown to improve FP implementation:
-
Multidisciplinary oncofertility teams, including oncologists, reproductive endocrinologists, mental health professionals, and nursing coordinators, have demonstrated improved referral rates and patient follow-through.8,14
-
Electronic health record (EHR) referral triggers, which prompt automatic fertility consultations for eligible patients starting gonadotoxic therapy, have effectively increased timely counseling.19
-
Structured provider education programs, especially in pediatric oncology, help improve clinician knowledge and confidence when discussing fertility risks and options.20
-
Standardized counseling checklists and decision aids: whether printed or digital, support consistent delivery of information and enhance shared decision-making during early treatment planning.1,17,21
-
Dedicated FP navigators or coordinators play a critical role in expediting scheduling, managing insurance authorizations, and facilitating interdisciplinary communication.17
While effective, these interventions remain unevenly implemented, particularly in low-resource settings. Broader integration into cancer care pathways and national quality measures is essential to ensure equitable access to FP across diverse hematologic oncology populations.
Novel Therapeutics and Emerging Concerns
The rapid evolution of hematologic cancer therapeutics presents unprecedented fertility counseling challenges not adequately addressed in existing oncofertility literature.
The advent of novel therapies in hematologic malignancies, such as chimeric antigen receptor T-cell (CAR-T) cell therapy, monoclonal antibodies, and targeted agents, has introduced new challenges in FP. While these therapies have significantly improved survival, their long-term effects on fertility remain poorly understood. In contrast to conventional high-dose chemotherapy and radiation, the gonadotoxic risks of which are well characterized, many novel agents lack robust human data regarding reproductive impact.14
This knowledge gap complicates counseling and decision-making. For example, CAR-T cell therapy is often preceded by intensive conditioning regimens, which are known to impair fertility, but the direct gonadal effects of the cellular therapy itself are still unclear.14,22 Similarly, the gonadotoxic potential of immune checkpoint inhibitors and tyrosine kinase inhibitors remains largely speculative, relying on preclinical data or isolated case reports.23,24
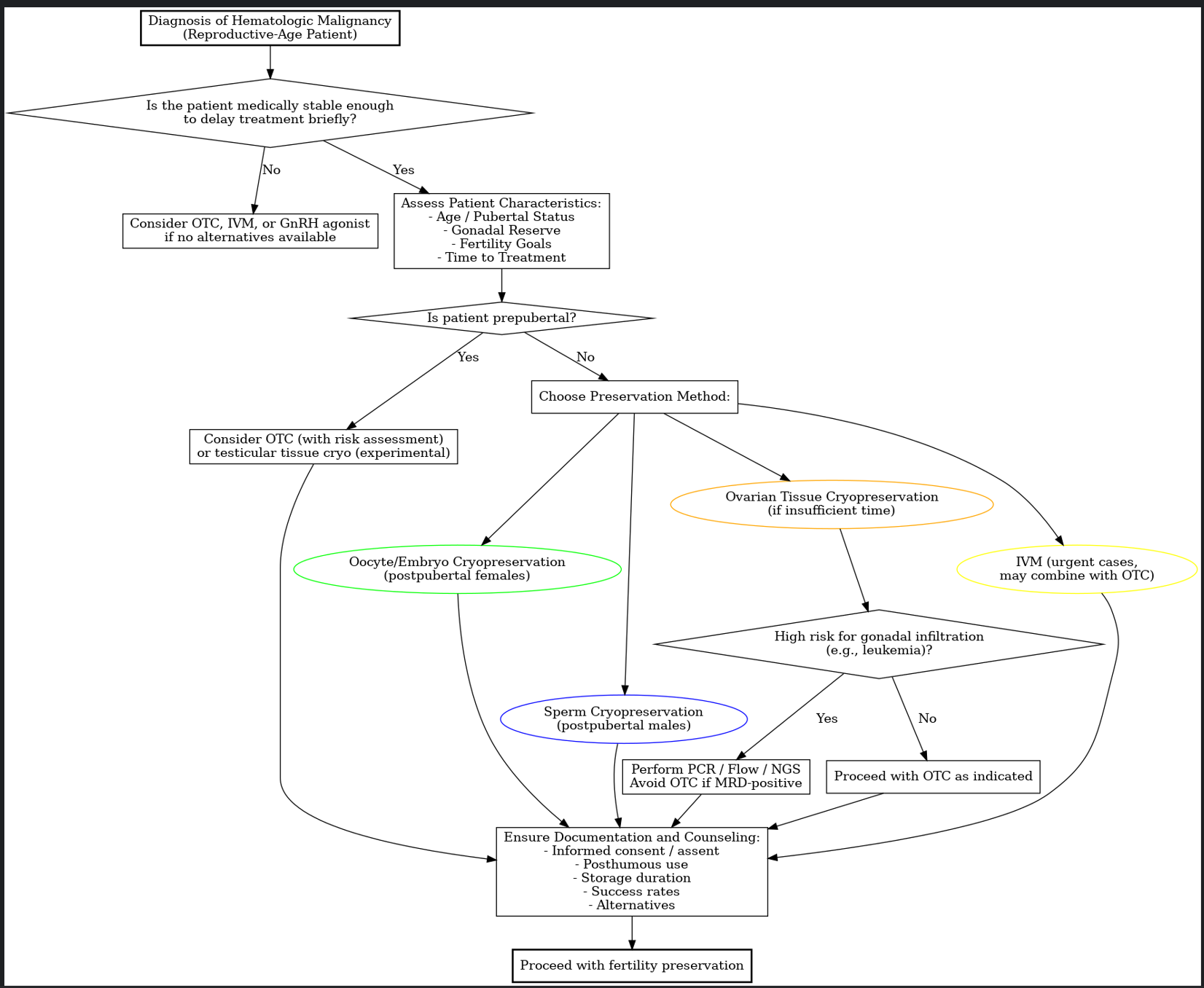
ASCO guidelines emphasize that FP should not be delayed by diagnostic workup or treatment staging if the patient is clinically stable. Timely counseling should occur as early as possible, and FP procedures can often proceed in parallel with initial oncology care.1 For female patients, random-start ovarian stimulation protocols are preferred, allowing initiation at any point in the menstrual cycle with typical completion within 10–14 days. Progestin-primed protocols and double stimulation approaches (e.g., Shanghai protocol) provide further flexibility for patients with limited time prior to treatment.25,26
Sperm cryopreservation remains the standard approach for postpubertal males, while oocyte or embryo cryopreservation is the mainstay for females. These techniques remain applicable even as treatment paradigms evolve. The uncertain fertility risks posed by newer agents underscore the need for individualized counseling and ongoing research to refine FP strategies in the era of precision medicine.
Gonadotoxicity Profiles of Conventional and Novel Therapies
Established High-Risk Therapies
The gonadotoxic potential of cancer therapies varies widely based on drug class, cumulative dose, and patient-specific factors. The 2025 ASCO guideline update provides stratified fertility risk profiles, highlighting that alkylating agents, platinum compounds, and high-dose radiation pose the highest risk for permanent infertility in both males and females.1
Alkylating agents such as cyclophosphamide and busulfan represent the greatest fertility threat, with cumulative doses above 4 g/m² in males or 8-12 g/m² in females markedly increasing infertility risk.21 Similarly, radiation exposures exceeding 20-30 Gy to the pelvis or 15 Gy total body irradiation are associated with near-universal gonadal failure.27
Moderate-Risk Conventional Therapies
Platinum-based therapies, while moderately gonadotoxic, do not reach the high-risk thresholds of alkylating agents but have been associated with reduced live birth rates in female survivors.28 Anthracyclines and vinca alkaloids carry lower individual risk, with fertility effects more dependent on cumulative exposure and concurrent gonadotoxic treatments.24,29
Novel Agents with Uncertain Risk
For emerging therapies, most are currently classified as low or uncertain risk due to limited human data. These include tyrosine kinase inhibitors, immune checkpoint inhibitors, monoclonal antibodies, and antibody-drug conjugates.23,30 Fertility preservation is recommended before starting these treatments as a precaution, particularly when administered with known gonadotoxic agents. For clinicians navigating complex treatment combinations, Table 2. summarizes gonadotoxicity risk profiles, evidence levels, and tailored fertility preservation strategies for conventional and emerging hematologic therapies.
This evidence-graded framework provides hematologic oncology teams with immediate risk stratification tools, addressing both established gonadotoxic agents and emerging therapies with uncertain fertility impact.
Fertility Preservation Utilization and Reproductive Outcomes
Current Utilization Patterns
Despite increased awareness and improved infrastructure, actual use of cryopreserved reproductive material by patients with hematologic malignancies remains consistently low. Reported utilization rates range from 2.6%-21.5% for sperm, 3%-9% for oocytes, and 9%-22% for embryos, depending on study population and follow-up duration.32 For ovarian tissue, utilization rates vary from 6.9%-30.3% in broader cancer cohorts, though data specific to hematologic malignancies remain limited.3
Reproductive Success Rates Among Users
Among patients who pursue conception using preserved material, reproductive outcomes can be meaningful. Live birth rates vary by preservation method: embryo cryopreservation yields 35-41% success rates, oocyte cryopreservation achieves 26-32%, and ovarian tissue transplantation results in 21-33% live births.3 These rates are consistent with outcomes in broader oncology populations but may be lower in patients with prior hematopoietic cell transplantation.
Factors Influencing Utilization and Outcomes
Low utilization rates reflect multiple factors including spontaneous fertility recovery, changes in reproductive goals, disease relapse, health deterioration, or successful natural conception. Among those who do pursue pregnancy, 22%-62% achieve conception, with most pregnancies occurring spontaneously rather than through assisted reproduction.2,33
Prior hematopoietic cell transplantation significantly impacts outcomes, with patients experiencing lower ovarian response, reduced oocyte yield in subsequent IVF cycles, and decreased pregnancy success compared to those who did not undergo transplantation.3
Psychological Benefits Beyond Reproductive Use
Importantly, even patients who never use preserved material often report significant psychological benefits, describing fertility preservation as providing ‘hope’ and ‘control’ during cancer treatment.13 These patterns underscore that fertility preservation serves as both a reproductive safeguard and a source of psychological reassurance. Current ASCO guidelines emphasize this distinction and continue to recommend preservation even when spontaneous fertility recovery is possible.1
Storage Duration and Management
The storage and long-term management of cryopreserved gametes, embryos, and ovarian tissue for FP are governed by institutional policies and national regulations which vary considerably across jurisdictions. These policies influence not only the logistics of storage but also patient decision-making regarding future reproductive use.
In the United States, there is no federally mandated maximum duration for storage of reproductive material. As per ASCO and ASRM guidelines, indefinite storage is permissible as long as institutional policies and patient preferences are respected. Annual consent renewal and explicit directives regarding disposition in the event of death or loss to follow-up are strongly recommended to ensure legal clarity and ethical transparency.1,34,35
In the United Kingdom, the Human Fertilisation and Embryology Authority (HFEA) previously enforced a 10-year storage limit. However, legislative changes in 2022 extended this limit to up to 55 years for patients with medical indications, including cancer. Continued storage now requires periodic consent renewals, which aim to balance reproductive autonomy with oversight.36,37
Other countries have adopted various approaches. Many European nations permit storage durations ranging from 10 to 20 years, often contingent on periodic consent and storage fees. In low- and middle-income countries (LMICs), regulatory frameworks are often underdeveloped or absent, and institutional policy may serve as the default governing standard. The International Federation of Gynecology and Obstetrics (FIGO) supports long-term storage on ethical grounds, emphasizing that reproductive cells and tissues can remain viable for extended periods without functional degradation.38
Across all settings, best practices call for robust informed consent protocols, annual patient communication, and documentation regarding storage intentions, particularly in cases of survivorship, patient loss to follow-up, or death. These practices are essential to uphold ethical and legal standards and to safeguard patients’ reproductive autonomy.1,35,37
Eligibility Criteria and Risk Stratification
FP decisions in hematologic malignancies must be tailored to individual patient factors including age, disease type, ovarian reserve, urgency of treatment, and the risk of malignant cell contamination in reproductive tissue. The ASCO 2025 guidelines endorse OTC as an established FP method, particularly for prepubertal girls and patients unable to delay treatment for ovarian stimulation.1
Success rates for OTC are highest in patients under 40 years of age with preserved ovarian reserve, while outcomes decline with age and diminished function. Importantly, in acute leukemias, the possibility of ovarian infiltration by malignant cells, even when histology is negative, poses a significant risk for disease recurrence following transplantation. As a result, molecular screening is now considered essential prior to ovarian tissue reimplantation.
Advanced diagnostic modalities such as PCR for leukemia-specific markers, flow cytometry, and next-generation sequencing are increasingly recommended alongside histologic and immunohistochemical analysis. These tools improve detection of minimal residual disease and are becoming standard for high-risk populations.1,16,39–41
For chronic leukemias (e.g., CML, CLL), the risk of ovarian involvement is considered low. However, OTC should still be preceded by molecular screening where feasible. In myelodysplastic syndromes and aplastic anemia, infertility risk arises primarily from the conditioning regimens used for Hematopoietic Cell Transplantation (HCT), rather than from direct gonadal infiltration. In these contexts, standard FP methods such as oocyte or embryo cryopreservation are generally appropriate.8,9,14,42–44
Eligibility decisions should therefore integrate clinical urgency, ovarian reserve testing (e.g., AMH), and disease-specific risks. For high-risk patients, particularly those with leukemia, molecular safety screening is a prerequisite to any consideration of ovarian tissue use. Table 3. presents diagnosis-specific fertility preservation recommendations, incorporating contamination risk, screening requirements, and age-adapted preservation strategies for patients with hematologic malignancies.
Emerging Technologies and Alternative Approaches
Emerging technologies are expanding FP options for patients with hematologic malignancies, particularly those for whom standard ovarian stimulation is not feasible due to time constraints or medical contraindications.
IVM is gaining traction as a valuable option for urgent FP. It allows retrieval of immature oocytes from unstimulated or minimally stimulated ovaries, followed by laboratory maturation and cryopreservation. IVM is especially advantageous for patients with hormone-sensitive disease, thrombocytopenia, or those requiring immediate chemotherapy initiation.9,46 While success rates remain lower than with conventional stimulation, IVM has led to successful pregnancies and is increasingly combined with OTC, as immature oocytes can be harvested from excised ovarian tissue and matured ex vivo before vitrification.9
In cases where no established FP method is feasible, gonadotropin-releasing hormone (GnRH) agonist co-treatment has been explored as a strategy to reduce chemotherapy-induced gonadotoxicity. Meta-analyses in breast cancer populations suggest that temporary ovarian suppression may reduce the risk of premature ovarian insufficiency and increase post-treatment pregnancy rates without compromising oncologic outcomes.47,48 However, evidence for efficacy in hematologic malignancies remains limited and inconclusive.
Recent data from long-term studies in young women with lymphoma indicate that GnRH agonists do not significantly protect ovarian function or enhance fertility outcomes when used during chemotherapy.49 As a result, current guidelines recommend that GnRH agonists should not be used as a standalone FP method. They may be considered only as adjuncts to cryopreservation, or when no other options are medically appropriate.49
These emerging strategies offer promising alternatives but must be applied selectively, with careful patient counseling regarding their experimental or adjunctive nature. Ongoing clinical trials and registry data are essential to clarify their role in hematologic oncology.
Disparities in Access and Ethical Considerations
Significant disparities persist in access to FP for patients with hematologic malignancies, driven by a combination of structural, financial, cultural, and institutional factors. In the United States, barriers such as insurance limitations, geographic location, and systemic racism disproportionately affect minoritized, rural, and low-income populations. Even in states with mandated insurance coverage, FP services are inconsistently offered, particularly to pediatric, adolescent, and male patients.17,50
Globally, FP infrastructure remains underdeveloped in many LMICs. Challenges include lack of trained personnel, absence of national guidelines, cost prohibitions, and limited availability of cryopreservation services. Cultural stigma, religious norms, and limited public awareness may further suppress demand or delay referrals.51–53 International surveys confirm that FP is often unavailable or unaffordable for cancer patients in LMIC settings.54,55
Fertility Preservation in Humanitarian and Conflict Settings
Fertility preservation in resource-constrained emergency settings, such as refugee camps, internally displaced populations, and conflict zones, represents one of the most acute equity gaps in global oncofertility policy. Oncology services in these settings are frequently suspended or under-resourced, while cryopreservation infrastructure, liquid-nitrogen supply chains, and trained reproductive specialists are virtually absent. The World Health Organization (WHO) and partners have urged that non-communicable-disease (NCD) care, including cancer and associated reproductive services, be embedded in all humanitarian response packages, citing the growing burden of displaced patients who require long-term management.56,57 For adolescents and young adults with hematologic malignancies, this translates into a “double jeopardy”: urgent gonadotoxic therapy delivered without the infrastructure or legal certainty needed for FP. FIGO’s oncofertility guidance explicitly calls for simplified, portable FP protocols (e.g., bedside sperm cryopreservation, ovarian-tissue extraction with delayed transport) that can be coordinated through regional hubs or mobile units, yet uptake remains minimal in active crisis zones.38 Policy solutions must therefore prioritize rapid referral pathways, cross-border tissue-transport agreements, and tele-oncology counselling to safeguard the reproductive rights of patients in humanitarian emergencies.
Fertility Preservation in Transgender and Nonbinary Patients
Fertility preservation in transgender and nonbinary (TGNB) patients with hematologic malignancies presents unique medical and psychosocial challenges. TGNB individuals may face barriers including lack of provider knowledge, gender dysphoria triggered by FP procedures (e.g., transvaginal ultrasound or masturbation for sperm collection), and inadequate institutional support. ASCO’s 2025 guidelines emphasize the importance of inclusive counseling that affirms gender identity, ensures informed decision-making, and addresses potential distress related to gamete retrieval or hormonal stimulation. Early, culturally competent FP discussions are essential, particularly before initiation of gender-affirming hormone therapy or gonadotoxic treatment. Oocyte or sperm cryopreservation remains feasible for most TGNB patients if appropriately timed and supported.1,17,58
Access inequities also extend to sexual and gender minority (SGM) individuals, who may face provider bias, lack of culturally competent care, or inadequate information about fertility options prior to treatment.1 These disparities underscore the need for healthcare systems to integrate FP into routine oncology care and develop equitable referral pathways.
Ethical Considerations
FP in hematologic oncology raises several ethical questions rooted in the principles of autonomy, beneficence, and justice. Patients are often confronted with high-stakes decisions under time pressure, compounded by uncertainty about prognosis and fertility outcomes. For minors, informed consent must involve a collaborative process of parental permission and child assent, with attention to developmental capacity and the child’s evolving autonomy.58 The American Academy of Pediatrics (AAP) encourages preserving the child’s “right to an open future,” especially when procedures are investigational.
FP in prepubertal children, particularly through ovarian or testicular tissue cryopreservation, raises additional concerns due to the investigational nature of these techniques and the absence of immediate reproductive intent. Unlike postpubertal patients, prepubertal individuals cannot produce mature gametes, making FP purely anticipatory and entirely reliant on future technological viability. These procedures require thoughtful counseling and multidisciplinary input to ensure decisions are ethically grounded and medically justified.
Posthumous use of reproductive material adds further complexity. The ASRM and AAP recommend that posthumous reproduction only occur when there is clear written authorization by the patient. In pediatric cases, posthumous use is not ethically supported unless the individual survives to legal adulthood and reconfirms consent.58,59 Institutional policies should mandate periodic re-consent for stored tissue and explicitly prohibit posthumous use without a documented directive. Ethical tensions intensify in cases where the child dies before reaching reproductive age, particularly when tissue was cryopreserved without their future input. Multidisciplinary ethics consultation is strongly advised in such scenarios to safeguard patient rights and uphold evolving standards of care.1,60
Risks associated with malignant contamination of preserved tissue, especially in leukemias, demand transparent discussion, multidisciplinary review, and meticulous documentation of risk mitigation measures. The principle of nonmaleficence requires that potential harms from tissue reimplantation be weighed carefully against reproductive benefits.9 To support clinical decision-making, Table 4 summarizes the primary ethical dilemmas encountered across patient populations undergoing fertility preservation in hematologic oncology, along with key considerations and recommended safeguards
Health Economic Implications
Beyond clinical and ethical considerations, fertility preservation in hematologic malignancies has important economic dimensions. Significant disparities in insurance coverage persist across countries and healthcare systems, with many patients—particularly in the United States and low- and middle-income countries—facing out-of-pocket costs for fertility consultation, cryopreservation, and long-term storage. Delayed referral can increase overall costs by necessitating emergency procedures or leading to missed preservation opportunities, which may later require more complex assisted reproductive interventions. Studies suggest that early FP counseling and referral are cost-effective when compared to post-treatment fertility interventions, especially in young survivors desiring biological parenthood. Integrating FP into routine oncology workflows and expanding insurance mandates can reduce long-term financial burden on both patients and health systems.17,54,55
Efforts to improve equity should focus on provider training, standardized referral protocols, insurance coverage advocacy, and culturally sensitive patient education. Internationally, integrating FP into national cancer care strategies and building capacity in underserved regions are necessary steps toward a more just and inclusive model of care.51–53

Posthumous Considerations
In the event of patient death, the disposition of cryopreserved reproductive material must follow explicit written directives established at the time of storage. Acceptable options include destruction, donation for research, or posthumous reproductive use by a designated partner, provided such use is clearly authorized. According to the ASRM, posthumous use of gametes or embryos is ethically permissible only when the patient’s written consent exists. In the absence of documentation, requests should only be considered if initiated by a surviving partner and reviewed under institutional policy.59
For pediatric and adolescent patients, the ethical framework is more restrictive. The AAP advises against posthumous reproductive use unless the individual survives to legal adulthood and can personally affirm or revise their directive. Consent forms should explicitly state whether tissue will be retained, discarded, or held for future decision-making upon reaching majority age.58
When no written directive is available, institutional policies and applicable legal frameworks guide disposition. In such cases, decisions should prioritize respect for presumed patient wishes. Regular review of consent documentation and legal oversight are essential to maintaining compliance with evolving ethical and regulatory standards. The American College of Medical Genetics and Genomics (ACMG) recommends that institutions maintain clear protocols for the storage and eventual disposition of postmortem reproductive specimens, including gametes and embryos.54,55
Requests for perimortem or posthumous gamete procurement, such as those arising in critical care or trauma settings, require urgent multidisciplinary review. Recommended participants in this process include reproductive specialists, palliative care providers, legal counsel, and institutional ethics committees, ensuring decisions align with patient rights, medical feasibility, and legal precedent.61
Conclusion
This review translates broad fertility preservation guidelines into specialized, actionable strategies for the unique clinical scenarios encountered in hematologic malignancies. By providing disease-specific algorithms, evidence-graded risk assessments, and practical tools for time-sensitive decisions, we address critical implementation gaps that have hindered optimal fertility preservation in this population.
Despite established guideline support from ASCO and other professional organizations, fertility preservation implementation in hematologic oncology remains inconsistent, with only 44% of hematopoietic cell transplant specialists routinely referring patients for consultation. Our analysis reveals that while provider counseling rates have improved from historical levels below 50% to 75-95% in specialized centers, significant implementation barriers persist: treatment urgency (cited by 83% of providers), limited pediatric options, sociodemographic disparities affecting minority and uninsured patients, and uncertain fertility risks of novel therapies including CAR-T cells and immune checkpoint inhibitors.
However, this review demonstrates that fertility preservation is both feasible and clinically meaningful in hematologic patients when disease-specific strategies are implemented. Key technical advances, including random-start ovarian stimulation protocols that enable preservation within 10-14 days, in vitro maturation for urgent cases, and molecular screening technologies (PCR, flow cytometry, next-generation sequencing) that improve ovarian tissue safety assessment—have expanded preservation options even under compressed timelines. Among patients who pursue conception using preserved material, live birth rates reach 35-41% with embryo cryopreservation and 26-32% with oocyte cryopreservation, demonstrating meaningful reproductive potential.
Our disease-specific risk stratification framework addresses the most critical decision-making challenges in hematologic oncology: distinguishing high-risk acute leukemias requiring molecular clearance before ovarian tissue use from lower-risk chronic diseases where standard preservation methods are generally safe. The clinical algorithms and evidence-graded recommendations provided here enable immediate implementation of appropriate preservation strategies based on diagnosis, treatment urgency, and contamination risk.
Priority interventions to improve fertility preservation equity and access should focus on: (1) standardizing early counseling protocols through electronic health record triggers and multidisciplinary oncofertility teams, (2) expanding access to time-sensitive techniques including in vitro maturation and emergency stimulation protocols, (3) implementing routine molecular screening for tissue safety assessment in appropriate patients, and (4) addressing persistent sociodemographic disparities through insurance coverage advocacy, provider education, and culturally competent care delivery.
Fertility preservation in hematologic oncology should no longer be viewed as optional or unfeasible due to treatment urgency. With the specialized strategies, risk-stratified protocols, and implementation tools provided in this review, fertility preservation can and should become a standard component of comprehensive cancer care that upholds the reproductive autonomy and future possibilities of all patients facing treatment for blood cancers. The clinical frameworks presented here provide the foundation for consistent, evidence-based fertility preservation that acknowledges both the unique challenges and remarkable therapeutic advances defining contemporary hematologic oncology practice.
Practical Relevance
The Clinical Application Box distills key evidence-based actions that hematologists, oncologists, and reproductive specialists can implement immediately in their daily practice. Given the urgency, complexity, and emotional impact of fertility preservation decisions in hematologic malignancies, these concise recommendations serve as a quick-reference guide to support timely, ethical, and individualized care. By translating broad guidelines into concrete steps, this summary empowers clinicians to close implementation gaps and enhance reproductive outcomes for patients facing gonadotoxic therapies.
Competing Interests
ZS declares no competing interests. AN declares no competing interests. MM declares no competing interests.
Funding
This work was not supported by any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ Contributions
ZS: Conceptualization, literature review, manuscript writing, revision. AN: Critical revision, final approval. MM: Literature review, critical revision, final approval. All authors reviewed and approved the final manuscript.
Ethics Approval
Not applicable (narrative review of published literature).
Consent for Publication
Not applicable.
Data Availability
This is a narrative review with no new datasets. All data supporting the conclusions of this article are included within the article and its references. No new datasets were generated during this study.
Acknowledgments
The authors thank the research teams whose work contributed to the evidence base synthesized in this review.