Introduction
Allostasis, defined as the process of achieving physiological stability through adaptive change, was first conceptualized by Sterling and Eyer in 1988 as a framework for understanding how organisms respond to changing environmental and psychosocial demands.1 McEwen and Stellar subsequently introduced the concept of allostatic load (AL) to describe the cumulative physiological wear and tear resulting from repeated or prolonged activation of these adaptive systems.2 Allostatic load is commonly operationalized as a composite of biomarkers spanning cardiometabolic, inflammatory, neuroendocrine, and related physiological domains.3,4 Higher AL reflects multisystem biological dysregulation and has been associated with poorer health outcomes in general adult populations.5
The relevance of AL in reproductive medicine is biologically compelling. Normal reproductive function, including folliculogenesis, implantation, placentation, and parturition, requires finely coordinated neuroendocrine, immune, and vascular signaling. Dysregulation may interfere with reproductive function through multiple pathways, including disruption of hypothalamic-pituitary-gonadal signaling, impaired folliculogenesis, altered endometrial receptivity, and adverse effects on placentation and parturition.4,5 Psychosocial stress is commonly experienced by individuals undergoing fertility treatment,6 and the ESHRE guidelines recommend routine psychosocial care as an adjunct to fertility treatment.7 However, biomarker-based physiological stress metrics are not currently operationalized in routine fertility or obstetric guidelines.
A growing body of empirical literature has begun to examine AL in reproductive contexts, spanning preconception cohorts, infertility treatment populations, and pregnancy outcome studies. However, this evidence base is characterized by substantial heterogeneity in AL definitions, with biomarker panels ranging from five to twelve components and scoring algorithms varying from clinical cutoffs to percentile-based worst-quartile counts, z-score sums, and latent class assignments. This variability makes cross-study comparison difficult and currently renders meta-analytic synthesis infeasible.
An additional methodological challenge unique to reproductive medicine is the timing of measurement. Pregnancy induces large trimester-specific physiological changes in blood pressure, lipid concentrations, insulin sensitivity, renal hemodynamics, and inflammatory markers.8,9 Therefore, AL biomarkers measured during gestation may reflect proximal gestational adaptation rather than pre-existing chronic physiological dysregulation, raising important questions about construct validity.
The present review focuses on infertility, assisted reproductive technology (ART), and pregnancy outcomes, where the evidence base and methodological challenges are most directly clinically actionable. The objectives of this narrative review are to synthesize available evidence on AL and reproductive endpoints, spanning infertility, fecundability, ART outcomes, and pregnancy complications; characterize methodological heterogeneity in AL operationalization across reproductive contexts; evaluate measurement validity concerns specific to pregnancy; and propose a harmonized, modular AL biomarker framework to reduce heterogeneity in future studies and enable evidence accumulation for clinical translation.
Materials and methods
Protocol registration and reporting
This narrative review was conducted without prospective protocol registration. Because formal registration and PRISMA-style reporting frameworks are primarily designed for systematic reviews, reporting was guided by the general principles of transparency, reproducibility, and good practice in narrative evidence synthesis.
Research question
This narrative review addressed the following guiding question: What is the available evidence on allostatic load across reproductive medicine contexts, spanning infertility, ART outcomes, and pregnancy complications? The review focused on individuals of reproductive age engaged in natural conception, infertility evaluation or treatment, including ART, or pregnancy. The exposure of interest was allostatic load, defined by any operationalized composite measure. The outcomes of interest included infertility and ART endpoints, including time to pregnancy, conception, clinical pregnancy, miscarriage, and live birth, as well as pregnancy outcomes, including hypertensive disorders of pregnancy, preeclampsia, preterm birth, small for gestational age or low birth weight, stillbirth, and composite adverse pregnancy outcomes.
Literature selection criteria
Eligible studies were published in English in peer-reviewed journals, reported an operationalized allostatic load composite with specified biomarkers and a scoring algorithm, and evaluated at least one reproductive endpoint from the prespecified outcomes of interest. Any allostatic load algorithm was accepted, including clinical cutoffs, percentile-based approaches, z-score composites, and latent class methods. Primary empirical studies and higher-level evidence syntheses, including systematic, narrative, and methodological reviews, were eligible if they provided substantial relevance to the interpretation of allostatic load in reproductive medicine. Non-human experimental studies, studies measuring psychosocial stress in the absence of an allostatic load composite, and conference abstracts without sufficient methodology were excluded.
Information sources and search strategy
This narrative review employed a focused literature search to identify studies evaluating allostatic load in reproductive medicine, including infertility, assisted reproductive technology, fecundity, and pregnancy outcomes. The aim of the search was to synthesize the available evidence and characterize methodological heterogeneity rather than to conduct a formal systematic review or meta-analysis. PubMed/MEDLINE, Web of Science, Scopus, and the Cochrane Library were searched from database inception to April 5, 2026. The search strategy combined terms related to allostatic load and reproductive outcomes, including allostatic load, chronic stress, infertility, assisted reproductive technology, pregnancy, preterm birth, preeclampsia, hypertensive disorders of pregnancy, fecundability, and adverse pregnancy outcomes. Searches were limited to English-language peer-reviewed publications. In addition, the reference lists of included studies and relevant review articles were manually screened to identify additional eligible publications through citation chasing.
Studies were eligible for inclusion if they reported an operationalized allostatic load composite based on physiological biomarkers and evaluated at least one reproductive endpoint or provided methodological insight relevant to the interpretation of allostatic load in reproductive populations. The reproductive endpoints of interest included infertility, fecundability, ART outcomes, hypertensive disorders of pregnancy, preterm birth, fetal growth restriction or small for gestational age, stillbirth, and composite adverse pregnancy outcomes. Eligible study designs included observational cohort studies, case-control studies, cross-sectional analyses, secondary analyses of randomized trials, systematic reviews, and narrative or methodological reviews relevant to allostatic load in reproductive medicine. Studies measuring psychological stress alone without an operationalized allostatic load composite measure were excluded. Animal studies and conference abstracts lacking sufficient methodological details were also excluded. Due to the heterogeneity in study design, biomarker panels, and outcome definitions, the findings were synthesized narratively rather than quantitatively.
Data extraction
Data from the included studies were summarized using a structured framework capturing bibliographic data, including author, year, country, and journal; study design; analytic sample size; population characteristics, including infertility diagnosis, ART versus natural conception, and gestational age at biomarker collection; allostatic load definition, including biomarker list, thresholds or scoring method, and directionality; reproductive outcomes, including definitions and ascertainment; covariates and confounding control; effect estimates with confidence intervals; missing data handling; reported limitations; and funding and conflict of interest statements. For studies that did not report full methods in the primary manuscript, supplemental materials were consulted where available.
Risk of bias and evidence grading
Study quality was appraised narratively, taking into account study design, sample size, potential for confounding, and measurement validity. To contextualize the strength of individual studies, each was assigned an evidence level using the Oxford Centre for Evidence-Based Medicine (OECBM) 2011 Levels of Evidence framework.
Synthesis
A narrative synthesis was undertaken, stratified by reproductive context, including infertility or ART, time to pregnancy or fecundability, and pregnancy outcomes, and by timing of allostatic load measurement, including preconception, first trimester, and mid-to-late pregnancy. A biomarker domain frequency analysis was also conducted to quantify the representation of each physiological system in primary empirical studies.
Results
Study selection
Literature searches identified 51 potentially relevant publications. After title and abstract screening, a full-text review was performed to determine eligibility. Thirteen studies met the inclusion criteria for this narrative synthesis, comprising seven primary empirical reproductive outcome studies, two construct-validity studies examining allostatic load measurement during pregnancy, one systematic review, and three narrative or methodological reviews relevant to the interpretation of allostatic load in reproductive medicine (Table 1). Additional studies were identified through citation chasing of the included articles and relevant reviews, and eligible publications from this process were incorporated into the final set.
Study characteristics
The included studies were published between 2013 and 2026 and were predominantly conducted in the United States, with most primary empirical studies originating from US-based cohorts. The included publications comprised a range of study designs, including primary empirical studies, construct-validity analyses, and review-level evidence. Among the primary empirical studies, the designs included a secondary analysis of a randomized controlled trial, prospective cohort studies, cross-sectional analyses, matched case-control studies, record-linkage cohort studies, and a latent-class cohort analysis. Sample sizes across the primary studies ranged from 42 participants with complete biomarker data to 4,266 participants in large prospective pregnancy cohorts.
Allostatic load composites varied substantially across studies, with biomarker panels ranging from five to twelve components and scoring approaches that included worst-quartile counts, z-score summation, clinical cutoffs, principal component analysis weighting, and latent class assignment. Cardiovascular markers, adiposity measures, lipid biomarkers, and inflammatory markers were the most consistently represented across studies, whereas neuroendocrine and renal biomarkers were less consistently included. This heterogeneity in biomarker selection, scoring algorithms, and measurement timing limited direct comparisons across studies and precluded quantitative synthesis.
Allostatic load in infertility and ART populations
The most direct evidence in an infertility treatment population comes from Barrett et al., who conducted a secondary analysis of the assessment of multiple intrauterine gestations from ovarian stimulation (AMIGOS) multicenter randomized controlled trial (n=836).10 Women aged 18–40 years with unexplained infertility undergoing ovarian stimulation with clomiphene citrate, letrozole, or gonadotropins had AL assessed at the preconception baseline using a 10-biomarker composite that included body mass index (BMI), waist-to-hip ratio, systolic and diastolic blood pressure, dehydroepiandrosterone sulfate (DHEAS), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides, C-reactive protein (CRP), and homeostasis model assessment (HOMA) score. Preconception AL was not associated with conception, spontaneous abortion, or live birth. However, among women who achieved a live birth, higher AL was associated with increased odds of preeclampsia and preterm birth, suggesting that in this cohort AL may have been more strongly associated with vulnerability during pregnancy than with fertility treatment success itself.
Complementary evidence from a cross-sectional analysis of National Health and Nutrition Examination Survey (NHANES) 2015–2018 (n=419; 59 infertile, 360 controls) found that AL was significantly higher in women with infertility than in controls after survey weighting.11 Subgroup analyses indicated that the association was stronger in non-smoking women, and BMI, LDL-C, triglycerides, HDL-C, and high-sensitivity (hs) CRP were identified as the biomarkers contributing most to elevated AL in the infertile group. However, the cross-sectional design precludes causal inference, and the infertility classification relied on self-report.
Allostatic load and pregnancy outcomes
Lueth et al.15 conducted a secondary analysis of the Nulliparous Pregnancy Outcomes Study: Monitoring Mothers-to-Be (nuMoM2b) prospective cohort (n=4,266).15 AL was assessed from 12 first-trimester biomarkers, including systolic blood pressure (SBP), diastolic blood pressure (DBP), cholesterol, LDL-C, HDL-C, hs-CRP, BMI, urine creatinine, urine albumin, triglycerides, insulin, and glucose, with high AL defined as four or more biomarkers in the worst sample quartile. High AL was present in 34.7% of participants and was associated with 50% greater odds of composite adverse pregnancy outcomes, including hypertensive disorders of pregnancy, preterm birth, small for gestational age, and stillbirth (adjusted odds ratio [aOR] 1.50, 95% CI 1.3–1.7). When individual outcomes were examined, the association was driven primarily by hypertensive disorders of pregnancy (aOR 2.5, 95% CI 2.0–2.9), with no significant association demonstrated for preterm birth or small for gestational age. High AL was also a significant partial mediator of racial disparities in hypertensive disorders of pregnancy. Notably, the inclusion of renal biomarkers and the full insulin-glucose axis represents an expansion beyond classic cardiometabolic AL panels, reflecting the specific pathophysiological relevance of endothelial dysfunction and insulin resistance in hypertensive disorders of pregnancy.
In a smaller matched case-control study (38 cases, 75 controls), AL measured before 15 weeks’ gestation using a nine-component pregnancy-specific index was substantially higher in women who later developed preeclampsia.16 Mean AL was 1.25 versus 0.83 (p=0.002), and the odds ratio for preeclampsia was 2.91 (95% CI 1.50–5.65) per unit increase in AL. AL also showed improved model fit compared with obesity alone.
Among prospective cohort studies focusing on preterm birth and small for gestational age, Wallace and Harville found that AL measured at 26 to 28 weeks’ gestation, based on five biomarkers including SBP, cholesterol, glycated hemoglobin, DHEAS, and cortisol, was associated with reduced gestational age.17 The adjusted beta was −0.18 (95% CI −0.35 to 0.00), providing early empirical evidence of an inverse association between AL and gestational age. However, mid-pregnancy timing of measurement is an important limitation, as noted by the authors.
Two cohort studies from the Bogalusa Heart Study using preconception biomarker measurements found no association between maternal preconception AL and the occurrence of preterm birth or small for gestational age, with or without neighborhood poverty as a contextual modifier.13,14 These null findings contrast with studies measuring AL in early pregnancy and suggest that biomarker panel composition, timing of measurement, or pregnancy-specific physiological pathways may influence observed associations.
Measurement validity in pregnancy
Two studies directly addressed the construct validity of AL when measured during pregnancy.8,9 Morrison et al.,8 analyzing pregnant participants from NHANES 1999–2006, found that AL biomarker values appeared to reflect proximal gestational physiological changes rather than lifetime chronic stress burden.8 Li et al.9 similarly explored gestational patterns of selected AL indicators and proposed a pregnancy-specific scoring approach incorporating gestational-age-adjusted reference values.9 Together, these studies underscore that AL algorithms calibrated in non-pregnant populations may misclassify or misrank pregnant women and that trimester-specific reference values or pregnancy-validated composite definitions are required for valid gestational AL inference.
Biomarker domain representation
Across the seven primary empirical studies for which sufficient biomarker detail was available, a systematic domain frequency analysis revealed near-universal representation of four physiological domains: cardiovascular markers in 7 of 7 studies, adiposity markers in 7 of 7 studies, lipid profile markers in 7 of 7 studies, and systemic inflammation markers in 6 of 7 studies. Insulin resistance and glucose metabolism were included in four of the seven studies, whereas the neuroendocrine domain was included in two studies. The renal domain was included in one study, the nuMoM2b analysis, exclusively in a pregnancy cohort in which endothelial dysfunction and renal physiology were directly implicated in hypertensive disorders of pregnancy. This pattern of domain representation motivates the harmonization framework proposed in this study.
Reviews and evidence syntheses
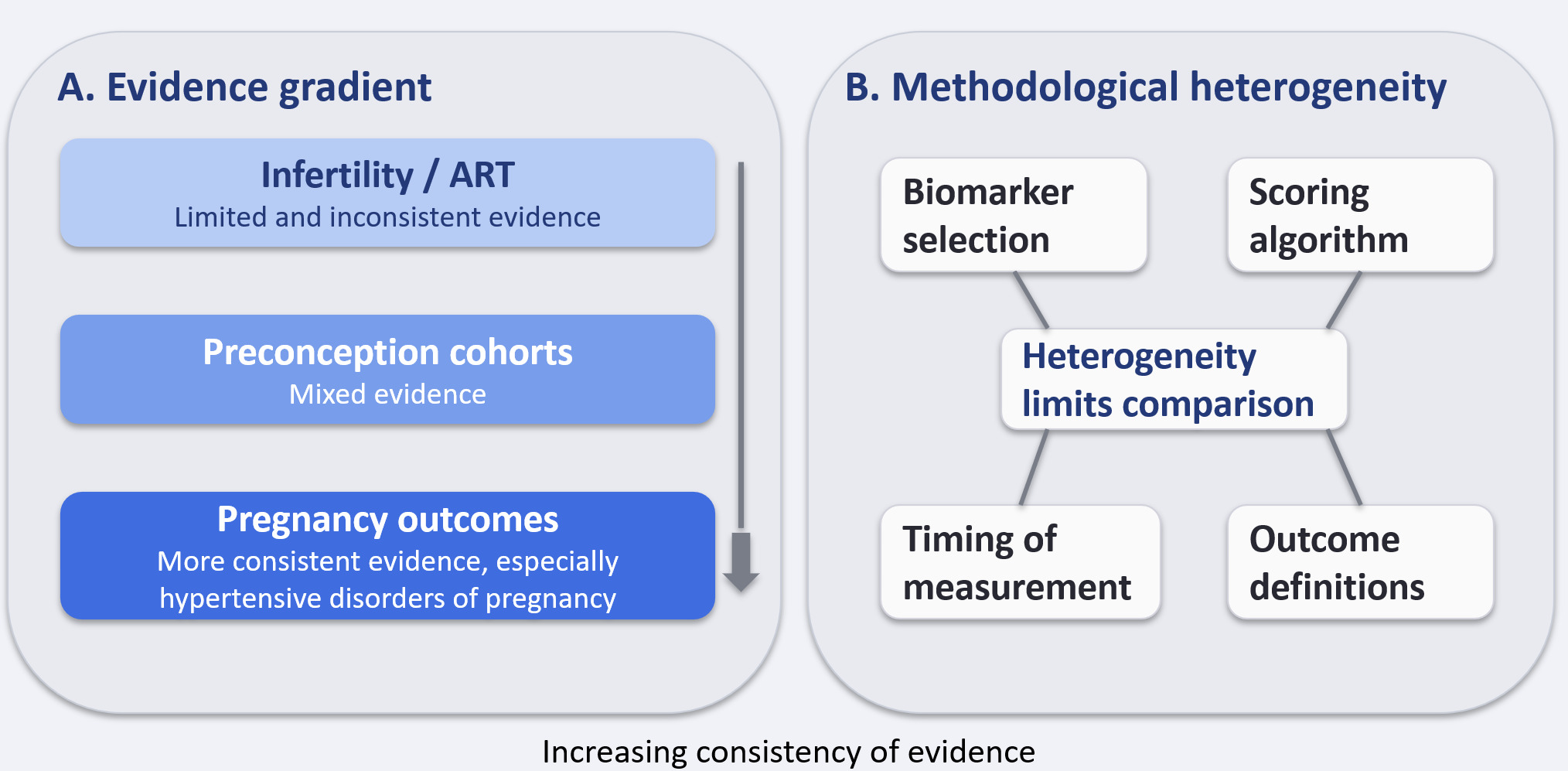
The 2022 systematic review by Premji et al. identified only three primary cohort studies meeting the eligibility criteria for prenatal AL and preterm birth.18 Sample sizes ranged from 42 to 156, and the authors concluded that heterogeneity in biomarker panels, scoring algorithms, and timing of collection, from 26 to 40 weeks’ gestation, precluded quantitative synthesis and limited interpretability. Narrative reviews by Olson et al.19 and Costello et al.20 contextualized AL within mechanistic frameworks linking chronic stress through neuroendocrine, inflammatory, and vascular pathways to adverse perinatal outcomes.19,20 Both highlighted trimester-sensitive biomarker interpretation as an unresolved challenge. The evidence gradient and principal sources of methodological heterogeneity identified across the included studies are summarized in Figure 1.

Discussion
Principal findings
This narrative synthesis identifies a limited but growing evidence base for allostatic load in reproductive medicine. Evidence linking allostatic load to infertility or fertility treatment success is inconsistent and limited. In contrast, several studies suggest that higher allostatic load is associated with adverse pregnancy outcomes, particularly hypertensive disorders of pregnancy, although findings for preterm birth and fetal growth outcomes remain heterogeneous. Substantial methodological variability in biomarker selection, scoring algorithms, and timing of measurement limits comparability between studies. In addition, construct validity concerns arise when allostatic load is measured during pregnancy, as physiological gestational changes may influence biomarker interpretation.
Clinical implications
The finding that higher preconception allostatic load was associated with adverse pregnancy outcomes but not with fertility treatment success in the only trial-embedded study identified to date has potentially important clinical implications.10 These findings suggest that allostatic load may serve as a marker of biological vulnerability to the physiological demands of pregnancy, based on the limited available evidence, rather than a barrier to conception per se.
Harmonised biomarker framework
Based on the domain frequency analysis and synthesis of methodological evidence, we propose a modular allostatic load panel for reproductive medicine research (Table 2). The core module, including blood pressure, BMI or adiposity, lipid profile (HDL-C, LDL-C, triglycerides), and CRP, represents the domains present in at least six of the seven primary empirical studies and provides a minimum comparability floor. An optional metabolic module, including HOMA of insulin resistance (IR) or fasting insulin and glucose, is recommended for studies examining insulin resistance pathways, which are particularly relevant to polycystic ovary syndrome and hypertensive disorders of pregnancy. The optional renal module, including albumin-to-creatinine ratio, is recommended for pregnancy cohorts with hypertensive disorders of pregnancy as a primary endpoint, given the direct role of endothelial dysfunction in preeclampsia. The optional neuroendocrine module, including DHEAS, hair cortisol, or salivary cortisol, is recommended when stress-system specificity is a study objective, acknowledging that many current allostatic load panels are dominated by cardiometabolic markers that may proxy overall metabolic health rather than cumulative stress.
For pregnancy cohort studies, we additionally propose that future studies consider assessing allostatic load at two time points: preconception, or first trimester at the latest, and, where feasible, the second trimester using trimester-specific reference values. This two-timepoint design would enable separation of pre-existing chronic physiological dysregulation from gestational adaptation, partially resolving the construct validity concerns raised by Morrison et al.8 and Li et al.9
The menopausal transition: an adjacent frontier
Although outside the formal scope of this review, the menopausal transition represents a biologically continuous extension of the reproductive allostatic load framework. Perimenopause is characterized by progressive shifts in the same physiological systems that comprise standard allostatic load composites, including rising blood pressure and visceral adiposity, adverse changes in lipid and glucose metabolism, increased systemic inflammation, and altered hypothalamic-pituitary-adrenal axis and autonomic regulation.22 Studies using the Study of Women’s Health Across the Nation cohort and related midlife datasets have reported associations between elevated allostatic load and vasomotor symptoms, sleep disturbance, accelerated cardiometabolic risk, and reduced functional health.23,24 The same methodological challenges identified in this review, including biomarker panel heterogeneity, inconsistent scoring algorithms, and the need for hormone-status-adjusted reference values, apply with at least equal force in the menopausal context, where ovarian hormone withdrawal itself drives substantial physiological change. A modular harmonized allostatic load framework, such as the one proposed here for reproductive medicine, may therefore be extensible across the full female reproductive lifespan, from menarche through the postmenopausal years.
Research agenda
Several high-priority research directions emerge from this synthesis. First, prospective preconception cohort studies incorporating a standardized allostatic load panel and following women through fertility treatment and, if pregnant, through delivery are needed. Second, head-to-head comparisons of allostatic load scoring algorithms, including worst-quartile count, z-score sum, clinical cutoffs, and latent class assignment, are needed to establish whether the choice of algorithm materially affects the magnitude and direction of associations with reproductive endpoints. Third, because nearly all primary studies in this review were conducted in the United States and focused on Black-White racial disparities, international replication in ethnically diverse populations is essential. Fourth, mechanistic studies examining the extent to which allostatic load predicts reproductive outcomes through specific biological pathways, such as inflammatory, vascular, and endocrine pathways, could identify modifiable targets. Fifth, intervention studies to determine whether allostatic load reduction, through lifestyle modification, stress management, or targeted pharmacotherapy, improves reproductive outcomes should be a translational priority. Sixth, extending the harmonized allostatic load framework across the female reproductive lifespan, including the menopausal transition, would enable longitudinal characterization of cumulative physiological wear and its potential clinical utility from preconception through midlife.
Strengths and limitations
To our knowledge, this is the first comprehensive narrative review to span allostatic load in infertility treatment, fecundability, and pregnancy outcome populations simultaneously, enabling an integrated view of the evidence landscape. The inclusion of a biomarker domain frequency analysis and a proposed harmonization framework provides actionable guidance for future study design.
This study has several limitations. The small number of primary studies identified, reflecting the early stage of this field, limits the strength of the conclusions that can be drawn, and effect estimates reported in individual studies should be interpreted with appropriate caution. Significant heterogeneity in allostatic load definitions, study populations, and measurement timing hampers direct comparisons between studies. Several studies used self-reported infertility or did not specify infertility etiology, introducing potential exposure misclassification. Publication bias cannot be excluded, given the small evidence base. Finally, the proposed harmonization framework is based on an expert synthesis of current methodological evidence and requires prospective empirical validation.
Conclusions
Allostatic load is an emerging and biologically plausible construct with potential relevance to reproductive medicine, spanning infertility, preconception health, and obstetric outcomes. Current evidence, although limited and methodologically heterogeneous, suggests that elevated allostatic load may be associated more consistently with adverse pregnancy outcomes, particularly hypertensive disorders of pregnancy, than with fertility treatment success. Evidence for associations with preterm birth and fetal growth outcomes remains mixed. Standardization of biomarker selection, scoring methods, and measurement timing, together with validation of pregnancy-appropriate allostatic load constructs, will be necessary before allostatic load can be meaningfully evaluated as a research or risk-stratification tool in reproductive medicine.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this manuscript, the authors used Claude AI (Anthropic), ChatGPT (OpenAI), Open Science AI tools, and Grok (xAI) for language editing and manuscript preparation. The authors reviewed and edited all AI-assisted content as needed and take full responsibility for the content of this article.
Conflict of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Ethical Considerations and Compliance
This study synthesized published literature and did not involve primary human subject data. Therefore, it did not require institutional review board approval. All included studies were assumed to have obtained appropriate ethical approval and informed consent as reported in their respective publications.
CRediT authorship contribution statement
Conceptualization: Yuval Or, Gideon Kopernik. Methodology: Yuval Or, Gideon Kopernik. Writing – original draft: Yuval Or, Gideon Kopernik. Writing – review & editing: Yuval Or, Gideon Kopernik.
Data sharing statement
No primary data were generated. All data supporting the findings are available in the studies cited in the reference list.