Introduction
Since the inception of Assisted Reproductive Technologies (ART), a substantial scholarly focus has been directed toward unraveling the intricate complexities of endometrial receptivity. This pursuit has culminated in many research endeavors dedicated to comprehensively assessing the characteristics of both embryos and blastocysts, coupled with meticulous evaluations of the endometrium, employing an array of methodological approaches.1,2
Traditional embryo characterization relies on meticulously analyzing microscopic attributes and their continuous developmental trajectory. Sophisticated methodologies, including time-lapse embryo monitoring, facilitate this investigation. A widely accepted classification system, initially proposed by Gardner and Schoolcraft, has become the standard for grading blastocysts, predicting successful ART cycles following embryo transfer.3,4 Additionally, recent attention has turned to Artificial Intelligence (AI) to determine the quality of oocytes and embryos/blastocysts for selection in uterine cavity transfer.5,6
In contrast, the realm of endometrial assessment continues to rely on ultrasonographic manifestations, supplemented by recent advancements in genetic investigations. This genetic exploration aims to define patient-specific implantation windows, thereby refining the timing of embryo transfer in the ART context.7,8 The scrutiny of the endometrial environment through ultrasonography has engendered extensive scholarly discourse, leading to a wealth of literature published in peer-reviewed scientific journals. These articles range from retrospective studies of thousands of cases to case reports and meta-analyses.9–12 However, this body of work presents diverse, occasionally inconsistent, conflicting outcomes, underscoring the intricate nature of this investigative landscape.
Two pivotal focal points have emerged from this literature. The first revolves around the multilayer architectural composition of the endometrium, particularly the identification of a trilaminar pattern and its implications. The second pivotal aspect pertains to endometrial thickness, especially during critical junctures such as human chorionic gonadotropin (hCG) administration before oocyte retrieval or the onset of progesterone supplementation in oocyte donation cycles and scenarios involving cryopreserved embryo transfer.13,14
While consensus emphasizes the significance of the trilaminar architecture in facilitating successful ART cycles, a notable divergence emerges when addressing endometrial thickness. Some experts advocate that dimensions exceeding 8 mm portend higher chances of ART success. In contrast, others propose that even modest thicknesses of 7 mm or less may support viable embryo implantation and favorable pregnancy outcomes.15,16 This diverse landscape of inquiry spans comprehensive studies involving substantial patient cohorts to intricate case reports, yielding variegated and occasionally conflicting conclusions.17 Furthermore, certain studies have posited that endometrial thickness may predict placental health and neonatal weight. At the same time, thin endometriums have been linked to adverse outcomes such as elevated spontaneous abortion rates, ectopic gestations, and placenta previa, among other possible obstetrical complications.18,19
The primary objective of our study is to introduce a fresh perspective on ultrasonographic endometrial assessment, unveiling an innovative classification framework that intricately elucidates its structural attributes. By illuminating this novel viewpoint, we aim to enrich the discourse within the field, foster a deeper understanding, and contribute to the overarching goal of refining ART practices and optimizing outcomes.
Material and Methods
This retrospective analysis evaluated ultrasound endometrial images from January 2018 to December 2022 of patients under 45 who underwent an autologous embryo transfer. Exclusion criteria encompassed subjects with cervical stenosis, prior uterine surgery, endometriosis, adenomyosis, known thrombophilia, patients harboring chromosomal rearrangements, cases using preimplantation genetic testing and using donor gametes or Maternal Surrogacy. Demographic characteristics such as age, body mass index (BMI), gravidity, and ovarian reserve metrics were collected. Cycle characteristics and embryologic data were recorded, including the total number of oocytes retrieved, number of mature oocytes (MII), oocyte maturity rate, fertilization rate, and blastulation rate. Participants were segregated into two groups: a-fresh embryo transfer and b-patients that underwent a frozen embryo transfer in a natural cycle.
Stimulation protocol
As previously described, patients underwent controlled ovarian hyperstimulation (COH) for IVF.20 Briefly, the COH protocol was selected at the discretion of the Reproductive Endocrinologist. It involved using follicle-stimulating hormone (FSH) and human menopausal gonadotropins (hMG) with a gonadotropin–releasing antagonist and human chorionic gonadotropin. Then patients underwent vaginal oocyte retrieval under sedation 35-36 hours post hCG administration.
Laboratory procedures
Embryo culture
All MII oocytes underwent intracytoplasmic sperm injection, and embryos were cultured to the blastocyst stage.20 Blastocysts were graded upon morphological criteria.3,4 For the fresh embryo transfer, one or two blastocysts at least class BB were selected, and the rest of the embryos, if viable, were vitrified.
Cryopreservation and rewarming techniques
These techniques have been described previously.20 After embryos were rewarmed, their survival was determined according to the appearance of blastomeres and zona pellucida and the ability of the blastocoel to re-expand. Degenerated embryos were deemed as failed to survive and not used for embryo transfer.
Endometrial preparation and Embryo transfer
To quantify endometrial thickness the maximal distance between the lateral margins of the midline longitudinal axis at the endometrium-myometrium interface was measured. For the assessment of architectural attributes, five key components were meticulously evaluated:
-
Well-defined hyperechoic external layers (a)
-
Thickness of the external layers (b)
-
Echogenic midline (c)
-
Hypoechogenic intermediate layers, positioned between external layers and the midline (d)
In both groups, the core intervention involved the transfer of two blastocysts, each meeting at least a BB classification as per the Gardner and Schoolcraft grading system.3,4 The timeline for embryo transfers differed slightly between the two groups: seven days after human chorionic gonadotropin (hCG) administration for fresh cycles and six days after the initiation of progesterone administration for the frozen cycles group. Ultrasound evidence ascertained pregnancy outcomes, specifically the detection of gestational sacs and embryonic heart motion approximately five weeks post-embryo transfer.
The assessment of endometrial configuration involved vaginal ultrasounds on two pivotal occasions: the day of hCG administration in fresh ART cycles treated with human menopausal gonadotropins and GnRH-antagonists and on the day of progesterone initiation in frozen embryo transfer cycles during spontaneous cycles. The timeframe spanning 2018 to 2022 saw the execution of this evaluation across four independent ART clinics. Endometrial images were captured during ultrasound sessions and subsequently centralized for meticulous analysis. The amassed data were aggregated and stratified based on the specific treatment regimens prescribed to each patient.
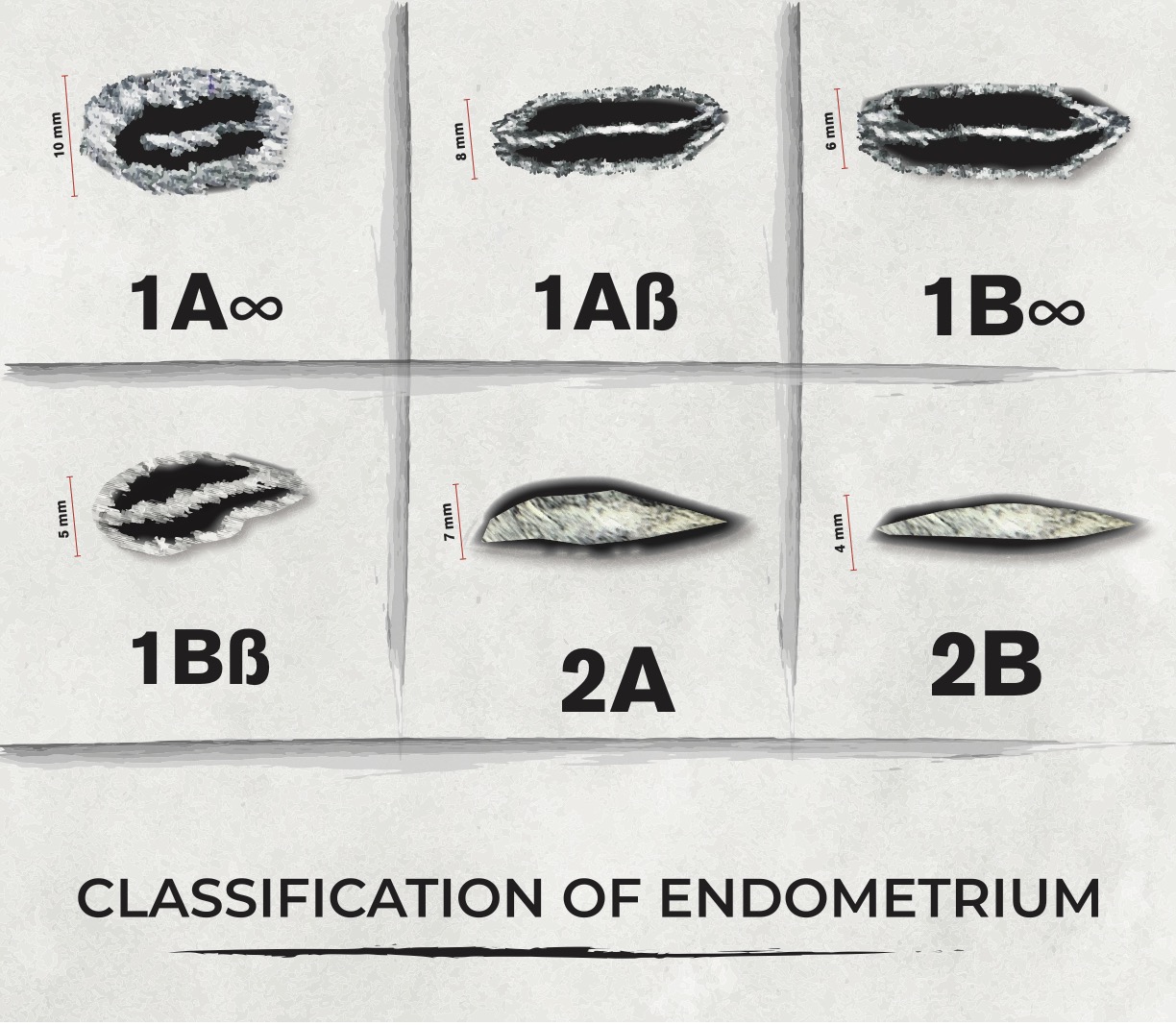
Leveraging these comprehensive endometrial attributes, we crafted a classification schema comprising six categories: I. Trilaminar configuration, equal to or exceeding 7 mm, with well-defined hyperechoic external layers comprising over 50% of the total endometrial thickness II. Trilaminar configuration, equal to or exceeding 7 mm, with well-defined hyperechoic external layers accounting for less than 50% of the total endometrial thickness III. Trilaminar configuration, less than 7 mm, with well-defined hyperechoic external layers equal or exceeding 50% of the total endometrial thickness IV. Trilaminar configuration, less than 7 mm, with well-defined hyperechoic external layers constituting less than 50% of the total endometrial thickness V. Non-trilaminar configuration, equal to or exceeding 8 mm, displaying increased hyperechogenicity compared to the adjacent myometrium VI. Non-trilaminar configuration, less than 8 mm, displaying heightened hyperechogenicity compared to the adjacent myometrium
Based on the aforementioned classification, a resulting grading system was established:
-
Trilaminar configuration: Yes (1), No (2)
-
Thickness: 7 mm or more (A), Less than 7 mm (B)
-
External layers: Equal to or greater than 50% of entire endometrial thickness α (Alpha), Less than 50% of entire endometrial thickness β (Beta)
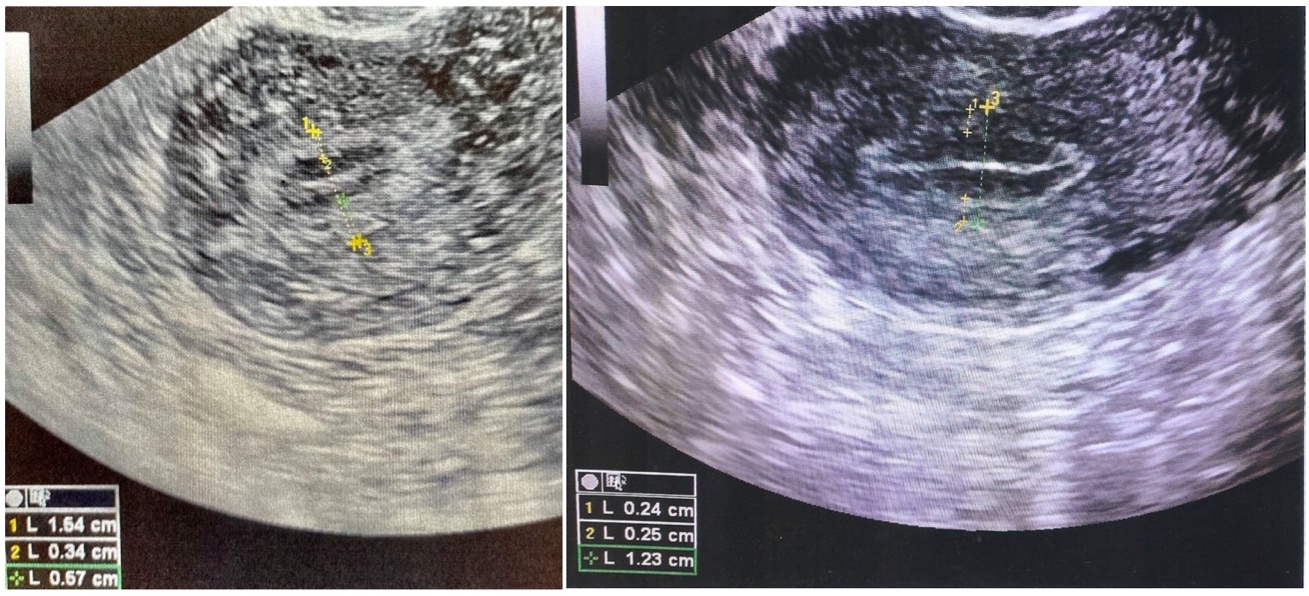
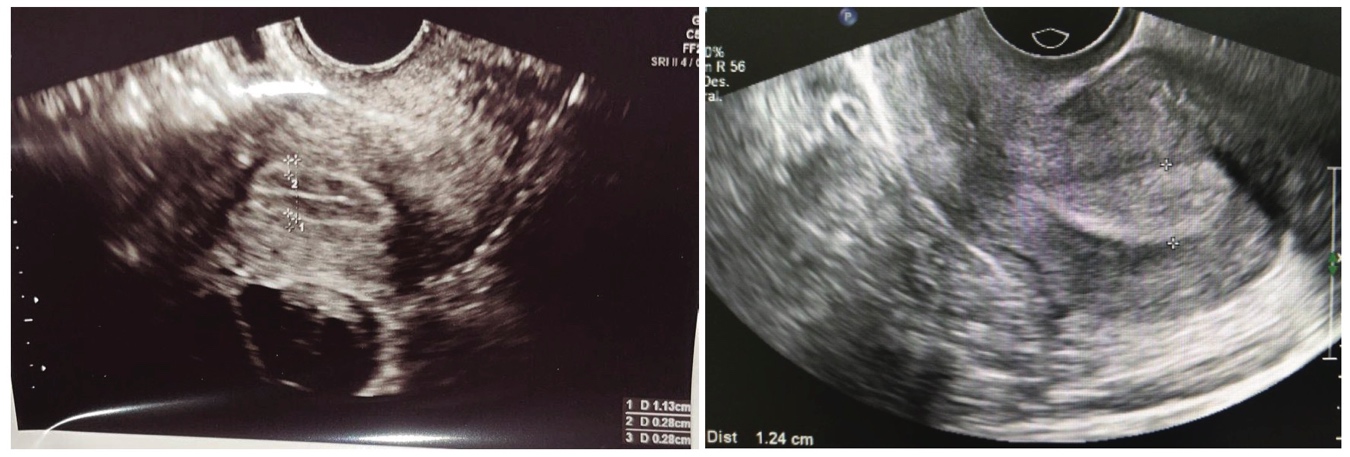
For a comprehensive visual representation of this grading system, refer to Figure 1. Additionally, to provide real-time examples of the diverse endometrial types, we present Photos 1 and 2. Our patient cohort comprised 271 individuals, categorized into two distinct treatment modalities:
-
Fresh cycles (141)
-
Frozen embryo transfer cycles (130)
The data analysis process involved the application of Student’s t-test and Chi-square test analysis to ascertain statistical significance between groups. This rigorous analysis allowed us to decipher meaningful insights from our observations.



Results
A total of 271 women underwent an embryo transfer. Group a: 141 and Group b: 130
The outcomes of this investigation unmistakably demonstrate a compelling correlation between the presence of amplified external endometrial layers, as identified through transvaginal ultrasound, and heightened pregnancy rates. This connection is particularly salient in instances where the endometrial thickness equals or surpasses 7mm.
Within the context of fresh in vitro fertilization (IVF) cycles as well as frozen embryo transfer cycles, the pregnancy rates exhibited a statistically significant elevation in the 1Aalpha subgroup when compared to all other groups (P < 0.05). Similarly, the pregnancy rates within the 1Balpha subgroup, while lower than the preceding 1Aalpha group, were still statistically superior to cases characterized by thinner external layers and endometrial dimensions (P < 0.05).
Noteworthy is the observation that patients attaining successful conception and delivery consistently manifested an endometrial thickness of 7mm, a consistent pattern observed across the 1Aalpha (α), 1Balpha (α), and 1Abeta(β)classifications.
In stark contrast, the outcomes of embryo transfers within the 1Aβ and 1Bβ categories markedly deviated with notably low success rates compared to all other groups, suggesting that embryo transfers in these cases may warrant reconsideration or cancellation.
Emphasis must be placed on the fact that no embryo transfers were conducted in patients lacking a trilaminar endometrial pattern. This decision was underpinned by our limited positive experience in treating such patients and the concurrent findings in existing literature.12
Examining the incidence of clinical twin pregnancies, we note the following rates: 11% and 10% for 1Aα and 1Bα in fresh cycles and 10% and 15% for 1Aα and 1Bα, respectively, in frozen cycles. Twin pregnancies did not transpire in cases where embryo transfers occurred within the 1Aβ and 1Bβ groups. It is pertinent to highlight that all twin pregnancies culminated in uncomplicated deliveries without chromosomal anomalies.
Regarding patient demographics, no statistically meaningful age disparities were observed between those who achieved conception and those who did not across all patient groups and diverse endometrial classifications.
A detailed breakdown of case distribution for each patient group based on treatment modality and subsequent classification of endometrial attributes is presented in Table 1. Meanwhile, Table 2 provides a comprehensive overview of absolute and percentage-based pregnancy occurrences across both groups, substantiating the statistically significant differences favoring cohorts characterized by thicker external endometrial layers.
Discussion
Let’s delve into the implications of our study’s findings. We’ve uncovered a significant correlation: individuals falling under the 1Aα and 1Bα categories demonstrated notably higher pregnancy rates. This intriguing link hints at a potential role played by the thickness of the external layers in augmenting endometrial receptivity.
In the realm of Assisted Reproductive Technology (ART), the visual assessment of endometrial characteristics through ultrasound imagery holds substantial implications for outcome predictions. While alternative techniques such as Doppler studies and genetic approaches have been explored to evaluate endometrial features, their precision and applicability have often fallen short. Notably, these methods failed to offer effective guidance for evaluating ART cycles, leading to their exclusion from recommended protocols outlined by esteemed bodies like the European Society of Human Reproduction and Embryology (ESHRE), and others.21,22
Our study introduces a paradigm shift in endometrial evaluation within ART cycles, employing ultrasonography as the primary tool. Diverging from convention, our observations present a distinctive perspective and propose a novel classification system. It’s important to acknowledge that while our classification system holds promise in its infancy, its refinement and validation by independent ART experts will be crucial steps in ensuring its robustness and reliability. In addition, further methods or technologies will be needed in the future to limit inter-observer variability and to evaluate endometrial images in a more robust interpretation.
In the broader context, we are drawn to the notable work of Greenwald et al.23 Their construction of a multidimensional atlas of the maternal-fetal interface delves into the intricate cellular composition of the endometrium, uncovering complexities that surpass the traditional focus on trilaminar patterns and overall thickness measurements. Similarly, the research conducted by Yamaguchi and colleagues employs advanced 3D imaging techniques to reveal previously concealed structural intricacies of the human endometrium.24 Their identification of the “rhizome” structure, an intricate network of endometrial glands extending along the myometrium, presents intriguing parallels with the external layer we identify through ultrasonographic observations. This prompts speculation that our externally identified layer might correspond to Yamaguchi et al.'s “rhizome” structure, aligning well with Greenwald’s segmented delineation.23,24 These correlations between the above mentioned studies and the results observed in the present report might explain potential underlying mechanisms that might explain the importance of the external layers proportions and endometrial receptivity.
Several limitations are important to mention about the present study. The number of cases was due to trying to maintain a homogeneous population without contaminating it with cases such as oocyte donation, sperm donation or maternal surrogacy, all of them factors that would need a more comprehensive multivariate analysis of the data. The present is an initial study that attempts to introduce a novel way to look at the phenomenon of endometrium characteristics as relate to its receptivity. Further studies to confirm the same results in cases of oocyte donation and maternal surrogacy are in our future horizon. We have attempted here to present a cohesive group of patients that fundamentally are autologous in terms of their own gametes and uterus.
The cutoffs of endometrial dimensions applied in this study reflect the majority of reports found in the literature by multiple authors. Due to the retrospective nature of the study and being multi-centric prevented us from doing a more sophisticated multivariate statistical analysis of the data.
At the heart of our study’s significance lies the introduction of novel parameters for ultrasonographic endometrial assessment within the context of ART cycles. This advancement transcends the conventional focus on trilaminar patterns and overall endometrial thickness, aspects that have historically stirred debates within the scientific discourse. Furthermore, the subjectivity and inter-observer variability associated with traditional evaluations underscores the importance of seeking more objective methodologies. While our findings hold substantial clinical implications, their ultimate validation through rigorous replication by diverse researchers is paramount. The accuracy and reproducibility of assessing endometrial characteristics by applying the new classification have to be confirmed by other technologies that will reduce the bias of the inter-observer interpretation. Should this validation transpire, the potential is substantial for an enriched clinical toolkit available to ART practitioners, grounded in a standardized and inventive endometrial classification framework that departs from established norms.
Conclusion
In conclusion, the application of a novel endometrial classification derived from ultrasonographic examination has yielded intriguing insights beyond the traditional considerations of total thickness and established patterns. The discernment of endometrial external layers and their relative proportions to the overall endometrial structure has unveiled a subgroup of patients undergoing In Vitro Fertilization (IVF) that exhibit notably augmented pregnancy rates, evident across both fresh cycles and frozen embryo transfer cycles.
However, it is imperative to underscore that the potential impact of this classification on enhancing pregnancy rates necessitates further consolidation through standardization and rigorous external validation. Replicating and substantiating these findings across diverse patient cohorts and clinical settings is a prerequisite for establishing the robustness of this novel classification’s association with improved pregnancy outcomes. This vital process will provide the requisite evidence to validate the clinical utility of the proposed classification framework within the context of assisted reproductive technologies.
As the boundaries of our understanding in this realm continue to evolve, our study contributes a stepping stone toward a more refined comprehension of endometrial dynamics in the context of assisted reproduction. The clinical implications of these findings could reshape practices and protocols, offering a more personalized approach to optimizing outcomes for patients undergoing ART procedures. Thus, continued collaborative efforts among clinicians and researchers are warranted to fully elucidate the significance of this novel classification and its potential contribution to enhancing reproductive success.
Conflict of interest
No conflict of interest exists among authors
Funding
There is no funding
Informed Consent Form
Not applicable
Authors Contribution per Credit
Conceptualization: Ricardo H. Asch Schuff (Equal), Tamar Alkon (Equal). Writing – original draft: Ricardo H. Asch Schuff (Equal), Tamar Alkon (Equal), Marlene L. Zamora Ramirez (Equal). Writing – review & editing: Ricardo H. Asch Schuff (Equal), Tamar Alkon (Equal), Marlene L. Zamora Ramirez (Equal), Jorge Suarez (Equal), Nicolas Laugas (Equal). Supervision: Ricardo H. Asch Schuff (Lead).