INTRODUCTION
In the US, there has been a dramatic increase in the use of intracytoplasmic sperm injection (ICSI) in combination with in vitro fertilization (IVF) over the past 15 years (1996-2012) from a staggering 36% to 76%.1 Similarly, in Europe, in 1998, the European Society of Human Reproduction and Embryology (ESHRE) reported the percentage of IVF and ICSI at 54% and 46%, respectively, but these percentages dramatically reversed over time until 2020 (last available data), when IVF accounted for 30% and ICSI for 70% of total annual procedures.2–4 Whether IVF/ICSI should be preferred to traditional IVF remains an open question, particularly with non-male fertility.5–7 ICSI is more invasive, expensive, and time-consuming than IVF but results in comparable live birth rates.7 A greater use of ICSI (in cases without male infertility) was propelled by reimbursement for the procedure by ART-mandated states.8 Overall, the expanded use of ICSI in couples with non-male-factor infertility shows “a gap between clinical practice and evidence”.7 The reported adjusted odds ratio for combined IVF/ICSI and birth defects in 3 meta-analyses from 1.32-1.37.9–11 The Practice Committee of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology’s most recent update in 2020 stated that ICSI has not demonstrated improvement in clinical outcomes in couples with non-male infertility.12 In light of these considerations, although traditional IVF is used less frequently both nationally and internationally than combined IVF/ICSI, it is imperative to understand the relationship between traditional IVF and birth defects due to a paucity of literature in this specific area.
Several previous published meta-analyses have revealed an increase in birth defects in children who were conceived through assisted reproductive technologies (ART), specifically consisting of combining both IVF and intracytoplasmic sperm injection (ICSI).9–11,13–15 In contrast, this systematic review and meta-analysis differs from earlier reviews because it focuses solely on IVF-conceived children and the risk of birth defects. Links between birth defects and IVF are poorly understood. Furthermore, recent improvements in IVF protocols in the past decade pose the question of whether the risk of birth defects has decreased over time.
Hence, the purpose of this review is to determine whether children conceived with traditional IVF are at greater risk for birth defects than naturally conceived children based on published studies through June 2023.
METHODS
This systematic review and meta-analysis consisted of secondary data analysis not involving human subject research and, thus, did not require an Institutional Review. We adhered to the preferred reporting items recommended by the “Meta-analysis of Observational Studies in Epidemiology (MOOSE)”.16
A search on PubMed and EMBASE databases was performed using the keywords birth defects, congenital malformations, IVF, and in vitro fertilization. EndNote X9.2 was used to manage retrieved citations. The search strategy is presented as a supplemental file, Appendix S1. The references from the obtained articles were further examined to identify relevant papers.
Description of Exposure, Outcome, and Study Population
In this systematic review and meta-analysis, IVF, the exposure, did not include any other ART procedures, including ICSI, zygote intrafallopian transfer (ZIFT), and gamete intrafallopian transfer (GIFT). Hence, our study population consisted of all IVF-conceived children and all naturally conceived children included in the selected studies. The primary outcome measures were any birth defects or congenital malformations, including major, minor, combined, or unspecified.
Eligibility Criteria and Study Selection
Inclusion criteria consisted of 1) original studies published in English, 2) those that reported pediatric birth defects for singletons after IVF treatment, 3) studies containing a naturally-conceived comparison group, and 4) prevalence rates or odds ratios. Exclusion criteria consisted of i) animal studies, ii) genetic studies, iii) reviews, iv) abstracts, case reports, and unpublished studies, v) IVF with oocyte donation, and vi) studies using other ART (e.g., ICSI, GIFT, ZIFT) as a comparison group.
Two investigators independently identified all relevant articles screening for eligibility using inclusion/exclusion criteria. Any disagreements were discussed and resolved among the two reviewers. The only disagreement between investigators pertained to the inclusion of two studies that were subsequently eliminated. Both studies, Olsen and Shevell, defined IVF with other ART procedures, including ICSI, ZIFT, and GIFT, respectively.17,18
Data Extraction
For each included study, data were extracted on author, year, country, study design, source of study sample, description of cases and comparison groups, exposure, predictors, outcome, results, and limitations (Table 1). For this systematic review and meta-analysis, the investigators only included relevant information on IVF exposure and birth defects as the outcome.
Quality appraisal of the evidence using STROBE criteria
To assess the quality of every study, STROBE criteria (Strengthening the Reporting of Observational Studies in Epidemiology) were employed by the two investigators. STROBE is an international, collaborative initiative of epidemiologists, methodologists, statisticians, researchers, and journal editors involved in conducting and disseminating observational studies to strengthen the reporting of observational studies in epidemiology.19
Nine selected items in the STROBE checklist were used to assess study quality, including: i) study objectives, ii) study design, iii) source of study sample, iv) participants’ characteristics, v) sample size, vi) quality of definition of exposure, vii) quality of definition of outcome, viii) results, and ix) study limitations. Quality assessment and final rating are reported in Table 2.
Each evaluation criterion was rated as “+” or “-,” depending on whether the study adequately did or did not, respectively, meet the specific criteria. When a "-"was assigned, an explanation was provided. The overall study was assigned a low, medium, or high-quality score based on the number of criteria that were rated as “-”. Hence, a high-quality study reflected no “-” scores, a medium-quality study reflected 1-4 “-” scores, and a low-quality study reflected 5 or greater.
The overall quality of each study was a reflection of the study authors providing thorough and detailed information in all categories that were directly related to the effects of IVF on birth defects. The paucity of relevant details was possibly a result of authors investigating other primary research questions. Hence, IVF and birth defects results may have been located in a sub-analysis in their publications.
Statistical Analysis
A descriptive analysis of the included studies was performed and presented in Table 1. Meta-analysis was conducted using STATA software, version 17, to calculate the pooled odds ratio for (i) all birth defects and (ii) major birth defects among IVF singletons compared to naturally conceived children. Pooled odds ratios were calculated using unadjusted odds ratios for “all” birth defects. Adjusted odds ratios were not used in this meta-analysis because of the convincing debate in the statistical literature about the appropriateness of combining adjusted odds ratios across studies. It states that if studies adjust for different covariates, then their adjusted odds ratios are not comparable.20
We also conducted a subgroup analysis for “major” birth defects. We performed sensitivity analyses to explore sources of heterogeneity and robustness by including one study at a time and recalculating the pooled effect estimates to assess the stability of results.
Heterogeneity was estimated using the I2 test and interpreted as the percentage of total variation across studies that is due to heterogeneity rather than chance. A value of >50% was indicative of substantial heterogeneity among the included studies.21 We used a random effect model to account for the expected heterogeneity among the studies due to differences in study populations, methods, and definitions. Egger’s test was used as a measure of asymmetry in the funnel plot, which may indicate publication bias or other small-study effects.
RESULTS
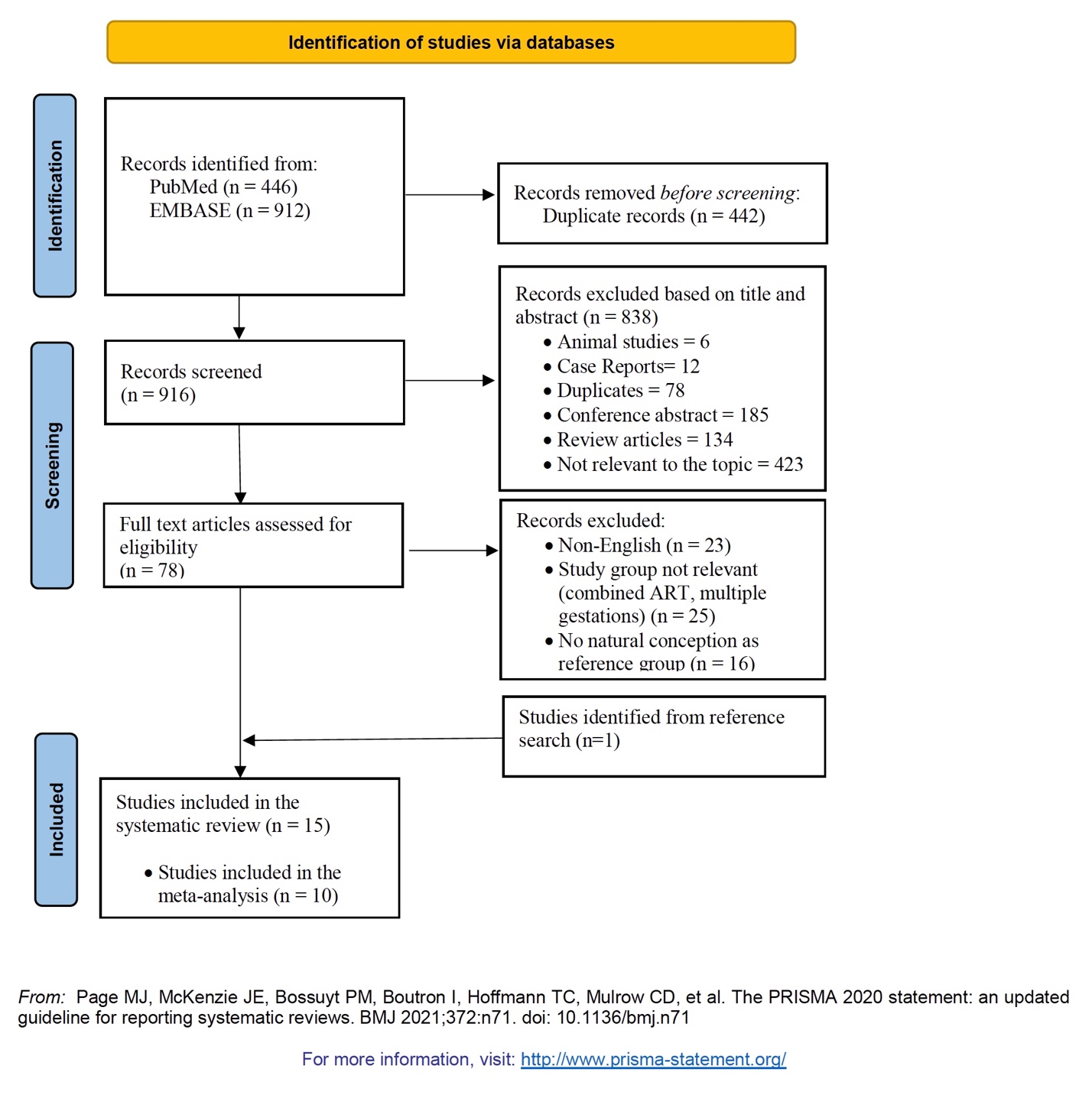
Figure 1 depicts the Preferred Recording Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram, mapping the number of studies identified, included, and excluded, and the reasons for exclusion.

After reviewing 916 articles, 78 full-text articles were reviewed against the eligibility criteria, and 64 were eliminated because they were not published in English (n=23), the study group was not relevant (n=25), and there was no natural conception comparison group (n=16). One relevant article was identified from references (Figure 1).
Ultimately, 15 relevant studies were included in the systematic review and meta-analyses.22–36
Study Characteristics
Of the 15 studies on birth defects and IVF, 8 studies were conducted in Europe22,23,30–32,34–36 and one each in China,33 Japan,27 Canada,25 and Israel.26 The remaining three studies were performed in Australia.24,28,29 A total of 8 studies had a retrospective cohort design,24–30,36 two were matched case-control studies,31,35 three were cross-sectional,22,23,27 and two were prospective cohort studies.32,33 The majority of studies were retrospective (66.67%), posing a high risk of bias. Most of the studies had sufficient IVF sample sizes ranging from 26236 to 15,570 patients,30 except for two studies with low sample sizes of 52 and 140, respectively.32,35 Information on birth defects was derived from birth or congenital malformations registries,28–31 hospital discharge registers,30 a perinatal database/registry/ies,22,25,27,34 researchers,33 parents reporting followed by a pediatrician’s general examination,23,32,35 ART centers,34 and a neonatologist.36
Timing of birth defects was diagnosed at birth or detected prior to release from the birth hospital,24,26,35 during the neonatal and/or perinatal period,22,27,36 at one year of age,28 at 4.5 or 5 years of age,23,32 or not disclosed.25,29–31,33,34 When assessing confounders, there was heterogeneity among the choice of potential confounders adjusted for in the multivariate analyses (Table 1).
Studies Reporting Significant Associations between IVF and birth defects
Table 1 contains details about STROBE criteria for each of the 15 studies.22–36 Table 2 summarizes the quality of each study with a rating from low to high. In both Tables 1 and 2, studies are presented by the most recent publication date.
Seven studies reported a statistically significant association between IVF and birth defects (Table 1).25,28–30,33–35 Results are presented from the newest to oldest studies. Qin reported a six-fold increased risk of congenital malformations in China (adjusted OR= 6.07; 95% CI: 3.14-11.72) while adjusting for a total of 22 potential confounders in 1260 children born with IVF compared to 2,480 naturally conceived children.33 A retrospective cohort study by Farhi conducted in Israel from 1997-2004 found an increased risk of congenital malformations in 1,680 IVF births compared to 202,935 spontaneously conceived live births (adjusted OR= 1.28; 95% CI: 1.00, 1.63).26
In Burgundy, France, between 2000-2009, Sagot and colleagues found an increased risk of congenital malformations (adjusted OR=2.0; 95% CI: 1.3=3.1) in IVF-conceived singletons (n=903) compared to naturally conceived children (n= 4,044).34
A slightly increased risk of congenital malformations (OR=1.15; 95% CI 1.07-1.24) was observed among 15,570 infants born after IVF versus 689,157 naturally conceived infants in Sweden during 2001-2007, after adjusting for year of birth, maternal age, parity, smoking, and body mass index.30
Data on 3,312 IVF (and 3,634 ICSI singleton pregnancies) were linked to perinatal birth defects occurring between 1991 and 2004 in Victoria, Australia, which were compared to 20,838 outcomes for singleton births.29 Overall, birth defects were increased after IVF (adjusted OR= 1.33; 95% CI: 1.14-1.55) relative to controls. A specific group, blastogenesis birth defects, were markedly increased among IVF children (adjusted OR= 3.24; 95% CI: 1.79-5.86) compared to the non-ART controls while adjusting for maternal age, year of infant birth, parity, and infant sex.29
In a Canadian retrospective cohort study, the subgroup analysis consisted of 319 IVF and 43,462 naturally conceived singletons.25 The prevalence of birth defects was highest among infants born with IVF (3.45%), compared to infants born with ovulation induction (2.35%), intrauterine insemination (2.89%), and spontaneous conception (1.86%).25
The prevalence of birth defects diagnosed in Australia within one year of age was significantly higher between 527 singletons born with IVF compared to 3,906 naturally conceived singleton children (adjusted OR= 2.20; 95% CI: 1.50-3.20) after adjusting for maternal age and parity, and sex of infant).28
Studies Reporting Non-Significant Associations between IVF and birth defects
The remaining 8 studies found no significant effect between IVF and birth defects.22–24,26,27,31,32,36
Risks of birth defects diagnosed before a child’s fifth birthday were compared in South Australian women who received treatment with ART to women who had spontaneous pregnancies.24 In a subgroup analysis, the increased risk of birth defects among IVF children (with fresh or frozen embryos n=1,484) compared to those children conceived naturally (n=293,314) was not significant (adjusted OR=1.07; 95% CI: .09-1.26) after adjusting for parental factors.24
Fujii and colleagues found no significant differences in congenital malformations between 1,396 singleton Japanese children born after IVF and 53,566 spontaneously conceived singleton children (adjusted OR=1.17; 95% CI: 0.81-1.69).27 In a European five-nation cohort study, no significant differences in odds of major malformations (assessed at 5 years) were reported for 437 IVF children compared to 538 naturally conceived children (adjusted OR=1.66; 95% CI: 0.70-3.95) after adjusting for social demographic differences.23
A Belgian study found no significant differences in the incidence of combined (major and minor) congenital malformations among 52 IVF children (9.6%) compared to 59 spontaneously conceived children (13.6%) (p= .787).32
In a retrospective analysis of 12,920 deliveries in Hungary, the incidence of major congenital malformations was not significantly higher (p>.05) among 262 IVF neonates (1.90%) compared to 262 matched naturally conceived neonates (1.15%).36
A study based on a Dutch national database between 1995 and 1996 reported that the adjusted odds ratio for the risk of any malformation for IVF children (n= 4,224 compared with naturally conceived children (n= 314,605) was 1.03 (95% CI: 0.86-1.23), after adjusting for maternal age, parity and ethnicity.22
No difference in congenital malformations was observed in four Dutch Hospitals among 307 IVF pregnancies compared to 307 naturally conceived pregnancies. (2.3%, 2.3%, respectively, no p-value provided).31
Finally, in a case-control study conducted in Belgium, there were eight (5.7%) minor congenital malformations at birth in 140 singleton pregnancies conceived by IVF compared to 140 matched controls (p<0.01).35 However, all the detected minor malformations spontaneously closed, resulting in this study’s conclusion that there were no significant differences between IVF pregnancies and spontaneously conceived ones.
Studies within the systematic review comparing fresh vs. frozen oocytes for IVF and ICSI and the risk of birth defects
Davies and colleagues evaluated the risk of birth defects among fresh IVF, frozen IVF, fresh ICSI, and frozen ICSI separately compared to spontaneous conceptions.24 Both fresh and frozen IVF and the risk of birth defects were not significant. In contrast, another study by Halliday and colleagues reported that both fresh (adjusted OR=1.43; 95% CI: 1.23-1.66) and frozen (adjusted OR=1.25; 95% CI: 1.04-1.52) embryo transfers using IVF vs. spontaneous conceptions were significantly associated with birth defects.29
Within our systematic review, four studies reported a statistically significant increased risk of birth defects after ICSI compared to spontaneous conception with adjusted odds ratios ranging from 1.40-2.54.26,28,29,31 Finally, Davies reported that fresh ICSI vs. spontaneous conception was significantly associated with the risk of birth defects (adjusted OR=1.73; 95% CI: 1.35-2.21).24
Quality of studies
A total of 8 studies were rated as high,22–24,26–29,33 while the remaining 7 studies were rated as medium quality.25,30–32,34–36 The most common reasons for the medium rating were: 1) the absence of diagnostic criteria or a classification system for birth defects, 2) only providing prevalence rates, and 3) the absence of adjusted odds ratios for birth defects among IVF-conceived infants compared to naturally conceived births. (Table 2).
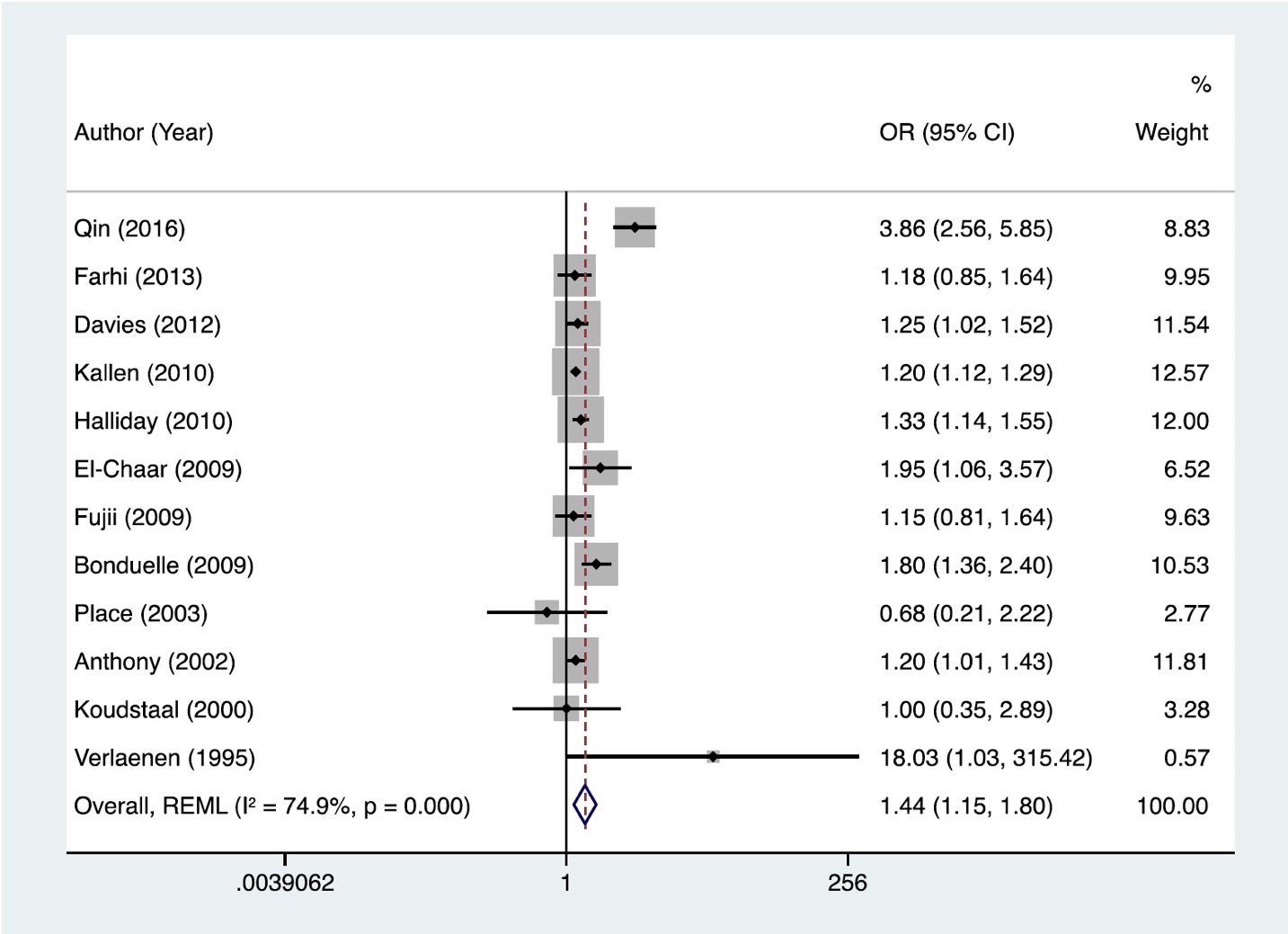
Risk of Any Birth Defects and IVF
A random effect model exhibited a statistically significant higher rate of any birth defects among IVF-conceived infants compared to naturally conceived singleton infants with a pooled odds ratio of 1.44 (95%CI: 1.15-1.80) (Figure 2). This model was chosen because the between-study heterogeneity was high (I2= 74.9%, p<.001). A visual examination suggested some funnel plot asymmetry; however, there was no small-study effect (Egger test, p = 0.14), supporting the absence of publication bias.

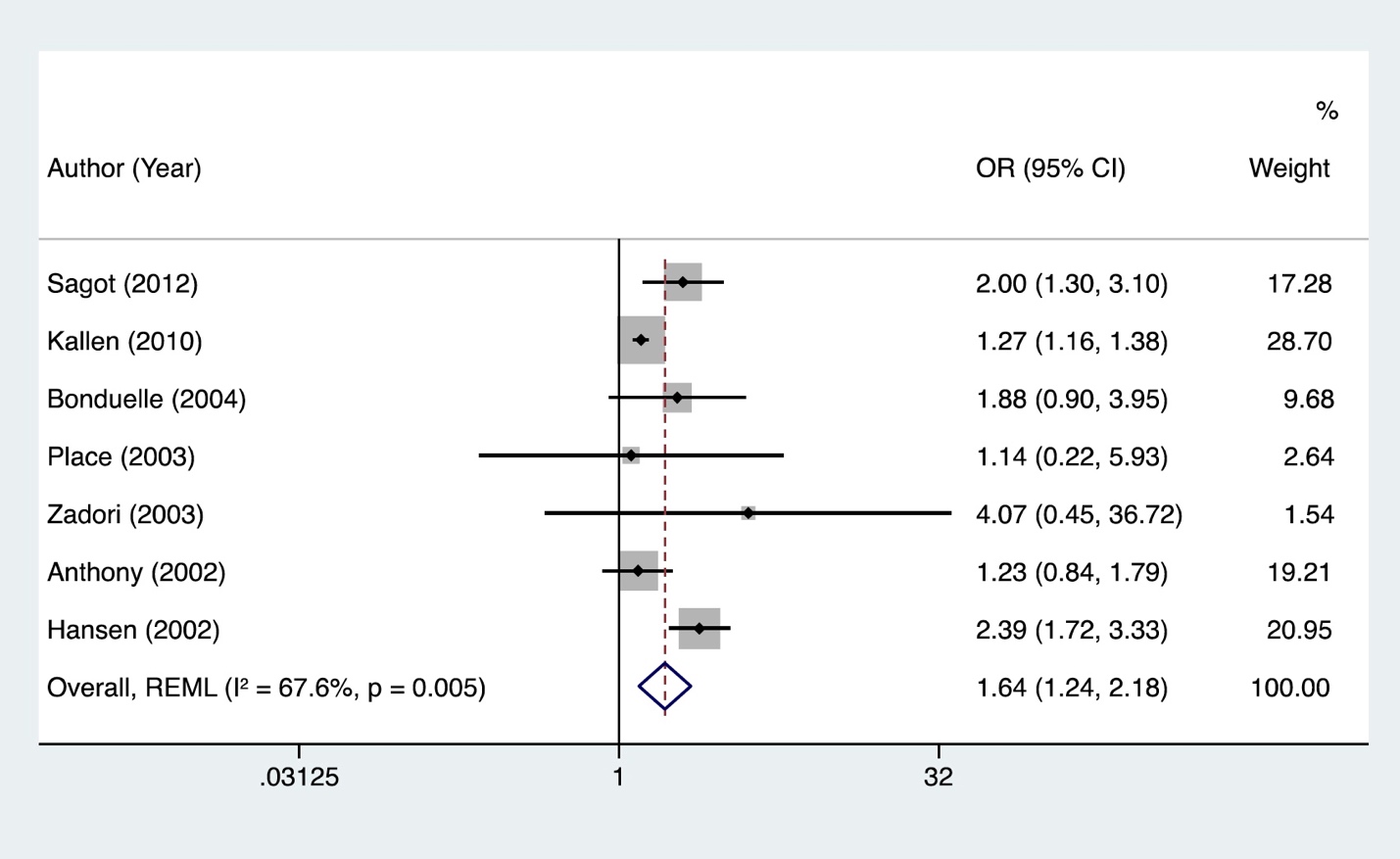
Risk of Major Birth Defects and IVF
Statistically significant heterogeneity was detected in the studies (I2= 67.6%, p=.005) and hence, a random effect model was used to calculate the pooled odds ratio. The IVF group has a significantly higher risk of major birth defects compared to naturally conceived children with a pooled odds ratio of 1.64 (95% CI: 1.24-2.18) (Figure 3).

Sensitivity analysis
The overall effect for the seven studies remained statistically significant in all sensitivity analyses when removing one study at a time, suggesting the robustness of the meta-analysis results. However, there was variation in heterogeneity based on which study was excluded. Most striking was when excluding the "Hansen (2002) study,"28 the overall effect was OR = 1.42 (statistically significant), and the heterogeneity decreased substantially: I² = 18.6% (low heterogeneity). In summary, we would conclude that the findings are generally consistent regardless of which individual study is removed, but the degree of heterogeneity among the studies does vary.
DISCUSSION
Our current systematic review and meta-analysis explicitly focused on IVF and all birth defects, consisting of a sample size of 30,171 singletons and 1,623,307 naturally conceived infants. Our study revealed an association between IVF and all birth defects with a pooled OR of 1.44 (95% CI: 1.15-1.80) among singletons. Additionally, the pooled OR for major birth defects was 1.64 (95% CI: 1.24-2.18) in a sub-sample of 21,901 IVF infants and 1,012,497 naturally conceived infants.
Existing Meta-Analyses
Six existing meta-analyses in the literature explored the relationship between combined IVF and ICSI technologies (referred to as ART) and birth defects, reporting either unadjusted or adjusted pooled odds ratios.9–11,13–15 Additionally, single and multiple births were often combined.
Three meta-analyses pooled adjusted odds ratios for birth defects among ART-conceived children (combining IVF/ICSI) ranging from 1.32-1.37.9–11 Only one study conducted by Zhao in 2020 that included a subgroup analysis, assessed whether traditional IVF procedures increased the risk of birth defects. Their results showed an increased risk of birth defects among IVF children (pooled RR=1.25, 95% CI: 1.12-1.40).14 In contrast to Zhao’s sub-group analysis, our study focused exclusively on IVF singletons and examined both “all” and “major” birth defects.
Postulated Mechanisms
Postulated mechanisms to explain the observed associations between IVF singleton pregnancies and birth defects include: i) advanced age of one or both partners of the infertile couple, ii) factors causing infertility in the mother or father, or prior treatment for infertility, iii) duration of infertility, iv) environmental exposures, v) chronic diseases such as obesity and diabetes, vi) risk behaviors such as alcohol, smoking, recreational drugs, and caffeine, vii) medications used to induce ovulation or to maintain the luteal phase, and viii) the IVF technology procedure itself, such as the culture media composition, the length of time in culture, freezing and thawing of embryos, the altered hormonal environment at the time of implantation, and the manipulation of gametes and embryos.9,10,15,23,24,28,33,37,38
It is well-established that subfertility, independent of ART treatment, is associated with poor infant outcomes.39 Women who struggled to conceive were 21% more likely to give birth to babies with birth defects compared to women who got pregnant without difficulty.40
Furthermore, patients diagnosed with infertility and opting for IVF may carry pathogenic genetic variants with variable expressivity, penetrance, and pleiotropic effects.41 On one hand, these genetic defects lead to sub- or infertility, and on the other hand, genetic errors may affect fetal development and cause birth defects. Alternatively, the parental genome may contain pathogenic genetic variants that predispose to increased mutability in embryogenesis (e.g., pathogenic variants in DNA repair genes). This includes ultra-rapid proliferation of cells (each round preceded by DNA replication) during a short timeframe. Finally, genetic sub/infertility may also increase the risk of DNA errors already in the germline leading to defective genomes in the oocytes or spermatogenic cells. Understanding and determining genetic causes of sub/infertility is extremely important but beyond the scope of our hypothesis for this systematic review and meta-analysis.
With regards to modifiable technical issues of IVF (e.g., medications, culture), there are considerable emotional, monetary, and time costs; hence, it is critical that this technique be optimized, and the risk of birth defects be decreased in the future.
Advantages and Limitations
The major advantage of our study pertained to the exposure, IVF, which was homogenous and did not include any other ART procedures, such as ICSI, ZIFT, and GIFT. When IVF was not the primary exposure, the odds ratios were retrieved from the subgroup analysis of the paper. It should be noted that there was sparse literature investigating the effect of IVF on birth defects. Only 47% of included studies in our meta-analysis utilized IVF solely as the exposure variable.22,27,28,33 The remaining studies all included other ART procedures (e.g., ICSI, ZIFT) with unadjusted odds ratios obtained from the sub-analyses of IVF and birth defects.
Our study had some potential limitations. First, it only included studies published in English due to a lack of resources which limited its generalizability. Second, the classification of birth defects was different across studies. Some studies included both major and minor malformations,22,30,32,33 while others only reported major,23,28,34,36 or minor malformations.35 Hence, our study separately examined the effects of IVF on “all birth defects” as well as “major birth defects”. Additionally, the majority of studies did not provide ICD codes for birth defects/congenital malformations.22–29,31–35
Different time frames for diagnosis of birth defects, specifically, at birth and/or hospital release,26 28 days,24 and 1 year28 were utilized in the studies. Thus, studies diagnosing malformations only at birth may ultimately have led to classification bias. In fact, for the identification of birth defects following IVF, a 1-year follow-up should be the minimum requirement, while 3 years would be the optimal length of follow-up in prospective studies balancing resources with complete ascertainment.42
In the future, larger and more homogeneous studies are required to evaluate our hypothesis. Additionally, geneticists/dysmorphologists should make the final birth defects diagnosis rather than pediatricians.
Potential confounders varied from study to study. We took the opportunity to peruse each study to determine whether there were differences (or patterns) with choices of potential confounders between statistically significant and non-significant studies, and two maternal characteristics and one infant characteristic emerged as the most common potential confounders. We found maternal age was included as a potential confounder in 86% of statistically significant studies25,26,28–30,33 compared to 50% of non-statistically significant studies.22–24,27 Likewise, parity was adjusted for 71% of statistically significant studies25,28–30,33 vs. 38% of non-significant studies.22–24 The sex of the infant was a confounder in 57% of significant25,26,28,29 and 13% of non-significant studies.24
Often, meta-analyses magnify biases and errors by including studies that are methodologically poor or that contain dubious results.43 Hence, the findings may not be definitive. Nevertheless, a critical review of evidence from meta-analyses for IVF and birth defects is important given their prioritization to inform clinical practice guidelines.44
Conclusions
In conclusion, this current systematic review and meta-analysis (as of June 2023) provide the highest available evidence for reproductive endocrinologists that IVF is associated with both “all” and “major” birth defects among singletons.
Future Directions
To better inform physicians and counsel patients, it is imperative to understand epidemiologic causes of birth defects among IVF singletons, including technical aspects of the IVF procedure, parental characteristics, and type(s) and causes of infertility.
Parental characteristics such as advancing age as well as past maternal medical history, including diabetes, cytomegalovirus, toxoplasmosis, varicella, rubella, and Streptococcus B are agents that are recognized to potentially cause birth defects in the developing fetus.45 Maternal psychological history, such as treatment of major depression with paroxetine, may increase teratogenic risk during natural conception46,47; hence, studies examining the risks of congenital malformations with first-trimester antidepressant exposure during in vitro fertilization should be explored. Lifestyle habits, including smoking alcohol, and illicit drugs including cannabis, and methamphetamine have been implicated in birth defects after natural conception.48–55 These risky behaviors could contribute to or confound the relationship between IVF and birth defects.
A greater understanding of the independent roles, particularly of modifiable contributors, as well as the interrelatedness of these factors, may hopefully lead to a decreased risk of birth defects following IVF in the future.
Finally, to obtain an accurate estimate of birth defects after IVF, future large prospective studies should employ standardized reporting and uniform protocols for identifying birth defects (e.g., photos) with consistent diagnostic criteria for both minor and major birth defects, and comparable durations of follow-up.
Conflict of Interest Statement
Hillary Klonoff-Cohen: None
Mounika Polavarapu: None
Disclosure Statement
Hillary Klonoff-Cohen: None
Mounika Polavarapu: None
Author Contributions
Conceptualization: Hillary Klonoff-Cohen (Lead). Methodology: Hillary Klonoff-Cohen (Equal), Mounika Polavarapu (Equal). Investigation: Hillary Klonoff-Cohen (Equal), Mounika Polavarapu (Equal). Data curation: Hillary Klonoff-Cohen (Equal), Mounika Polavarapu (Equal). Project administration: Hillary Klonoff-Cohen (Lead). Supervision: Hillary Klonoff-Cohen (Lead). Writing – original draft: Hillary Klonoff-Cohen (Equal), Mounika Polavarapu (Equal). Writing – review & editing: Hillary Klonoff-Cohen (Equal), Mounika Polavarapu (Equal). Formal Analysis: Mounika Polavarapu (Equal).
Details of ethical approval
This systematic review and meta-analysis consisted of secondary data analysis not involving human subject research and thus did not require an Institutional Review.
Funding
None