
Egg quality, particularly in older patients, is one of the most relevant and frustrating issues in assisted human reproduction. As a female enters advanced reproductive age, her baseline FSH increases, while age-associated ovarian fibrosis, characterized by collagen accumulation and structural stiffening, occurs.1 These concurring processes create a state of “double jeopardy” for the developing follicle, wherein follicles expand faster, while the diminished capacity of the cortex to accommodate this expansion causes follicles to lose their integrity at a smaller size. Together with an age-related increase in markers of inflammation, this inevitably predisposes older patients to premature spontaneous luteinization and rupture, which clinically manifests as shorter and irregular cycles.2 In addition, high-level FSH may directly damage the egg by competing for control of cumulus cells, which have only a limited number of FSH receptors and, under normal physiological conditions, unlike mural granulose, remain dedicated to nursing the egg. All issues affecting the reproductive cycle of older patients can be further exacerbated during ovarian stimulation since the physician must add exogenous FSH to make IVF attempts worthwhile.
Several approaches have come to the forefront of practice in the last decades to remediate this issue. First, it was proposed to minimize the amount of FSH used for ovarian stimulation – minimal stimulation (MS).3 MS has achieved moderate success and saves patients considerable money (per cycle) on medications. However, its obvious disadvantage is the small yield of eggs, which usually translates into more cycles required to achieve pregnancy. The recently proposed Highly Individualized Egg Retrieval (HIER) protects follicles and eggs by preemptively truncating the follicular phase before FSH can exert its damaging effect.4 With HIER, eggs are retrieved while the follicles are small and before they have a chance to luteinize. This simple and practical approach yields more eggs than minimal stimulation but is challenging to scale to a large number of patients because of an unpredictable retrieval day. Also, it produces a considerable percentage of immature oocytes, which must be matured in vitro, creating another obstacle to large-scale use of this approach.
Ironically, despite the general acceptance of at least a potential for the harmful effect of high levels of FSH in the circulation, there are not many systematic studies (other than those performed by a manufacturer) of circulating FSH during ovarian stimulation. FSH is almost never monitored during stimulation outside of research projects. Instead, during conventional stimulation, the physician relies exclusively on measuring the response to FSH: namely follicles number and sizes and the level of estradiol. Yet, these parameters have no prediction value for the circulating level of FSH; therefore, the “high level of FSH” has no actionable reference point. Furthermore, a lot about FSH levels remains a mystery. For example, if a female’s baseline FSH level is 17 mIU/mL, would an additional 4 mIU/mL be sufficient to rescue follicles? At what FSH level the saturation is reached when increasing FSH does not produce an increased response? Our experience of measuring FSH during ovarian stimulation shows that patients metabolize it at vastly different levels and, worse, in about 15% of patients, spikes to levels above 40 mIU/ml cannot be explained by the circulating level expected at the amount of administered FSH (Dozortsev et al, unpublished). The only thing we know for sure is that interpatient variability is considerable.5 This is why we believe that truly customized stimulation requires knowledge of circulating FSH and is one of the cornerstones of the latest addition to the “toolbox” of improving egg quality is named “Term Stimulation”- TS.6
“Term Stimulation” name is derived from the well-established OBGYN concept of term pregnancy and delivery. It implies the existence of a benchmark duration of the follicular phase that produces more competent oocytes, similar to term pregnancy, which produces a fully mature fetus. The concept of TS is rooted in epidemiological studies pointing to a decrease in the fecundity of females with shorter cycles, irrespective of age.6 Indeed, even in young females, the cycle duration reduction is accompanied by a dramatic drop in fecundity.7 Notably, the reduction is usually due to the shortening of the follicular phase, while the luteal phase remains relatively unaffected.8
Furthermore, extending the follicular phase has been shown to improve fecundity.9 Until recently, fecundity reduction in short cycles was attributed to a less competent corpus luteum. However, the advent of a frozen transfer, particularly “freeze all” cycles, made it possible to dissect the impact of a shorter follicular phase on egg quality from the impact of the luteal phase. It has to be mentioned that for accurate evaluation, the duration of stimulation must be an independent variable. This requires the inclusion of only those cases where stimulation was extended for random reasons, such as the patient’s sickness or her error in medication regimen, etc. Only such cases were included in the group of stimulation that lasted 13 days or longer in Table 1. As we can see, patients with prolonged stimulation do at least on par or perhaps better with extended stimulation. This can only be attributed to better-quality eggs since all embryos are transferred in frozen cycles.

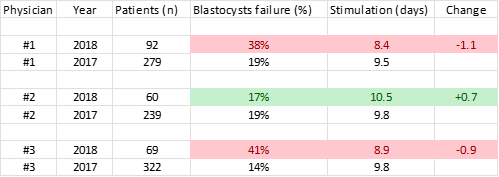
The existence of term stimulation does not imply that all eggs not reaching term will be incompetent. Just like many preterm newborns recover, many preterm eggs will become a viable pregnancy. However, there seem to be a cliff for the duration of stimulation - around 9 days, before which the percentage of eggs “born” competent sharply drops. Table 2 below illustrates this point. In this case, the clinic’s management was concerned that there was an apparent increase in canceled cycles in the first quarter of the new year due to the complete failure of blastocyst culture. An analysis presented in Table 2 reveals that it only affected patients of physicians 1 and 3. These physicians reduced the duration of stimulation to under 9 days because they believed it would improve egg quality. Embryos of the physician’s patients who had not changed the duration of stimulation remained unaffected. After reviewing the data, physicians #1 and #3 increased the duration of their stimulations, and their results reverted to the baseline.

Term stimulation is an approach to managing the ovarian cycle by extending it to a physiological duration in the most fertile population – about 17 days before LH surge.8 Term Stimulation is achieved by deciding on a day of the retrieval before starting FSH and maintaining circulating FSH within the range that paces follicular expansion to achieve the desirable size on the predetermined day.10 As an additional precaution against premature spontaneous luteinization, patients undergoing Term Stimulation may receive suppositories with 50 mg of diclofenac twice daily, in the last third of the stimulation, to suppress follicle inflammation.2,6
In the accompanying manuscript, Dr. Villar et al. report the details of two cases of term stimulation10 when the duration of stimulation was extended to 17 days. The first case describes a patient 42 years old, with two prior failures of IVF due to the lack of chromosomally abnormal embryos. This patient is currently in the 22nd week of an uneventful pregnancy. The second case describes term stimulation in a 37-year-old patient with two previous IVF failures due to poor embryo quality. This patient delivered a healthy child to term. One of the interesting points about those cases is that in the first case, the patient in her term stimulation cycle received more FSH than in her previous two failed IVF cycles. In contrast, a patient in the second cycle received considerably less. This indicates that the story may be more complicated than mere exposure to high FSH levels.
Chromosomal error is an objective, quantifiable benchmark of embryo quality. These errors are probably the most important obstacle to achieving pregnancy in older patients. Most of the chromosomal aberrations found in preimplantation embryos can be traced back to meiosis I or, in practical terms, to about one hr. interval after the trigger’s peak in the blood; until then, all eggs are chromosomally normal in all women, regardless of age. This means that whatever happens to the egg before or during the stimulation, including excessive FSH levels, can only predispose it to chromosomal errors, not directly cause them. It is an ovulation trigger that is a direct causing factor of chromosomal errors. Therefore, the nuances of triggering older patients may play an important role. To this end, we believe that a physiological ovulation trigger, progesterone, may improve the outcomes.2 Unfortunately, progesterone cannot be used as a trigger during conventional stimulation because its action requires an intact GnRH signaling pathway. However, we believe preventing premature ovulation with diclofenac or another anti-inflammatory drug may solve this problem.
Term Stimulation protocol requires much attention to detail, which makes it challenging to scale it manually. Therefore, so far TS has only been used in only 24 patients who had at least two prior IVF failures due to proven low egg quality and refused an egg donor option. At the same time, TS is easily digitizable. After about 1,000 patients, we hope to accumulate enough data to outsource term stimulation to AI, providing highly customizable and yet, easily scalable solution that allows to schedule the retrieval weeks in advance. Then, it could be expanded to all patients.
In conclusion, there is a strengthening consensus that ovarian stimulation has a profound effect on the quality of the oocytes and its duration has emerged as an important independent variable. Surprisingly, two seemingly irreconcilable approaches to duration of follicular phase demonstrate their benefits for improving egg quality in patients of advanced reproductive age. One of them, shortening of the follicular phase, is supported by clinical cases in older patients and, indirectly, by experience with in vitro maturation.11 The second, in contrast, extension of the follicular phase to its duration in the most fertile patients population has been also supported by clinical observations and extensive epidemiological data. The existence of such paradox usually implies a a gap of knowledge in underlying physiology and indicates that we may be on the verge of a major breakthrough, as this recently happened, when progesterone’s ability to, both, block and induce ovulation was finally reconciled with realization that it is a physiological GnRH agonist.2
Until then, the decision which of the two approaches may benefit a specific patient will remain empirical.
Authors’ Contribution per CRediT
Conceptualization: Dmitri Dozortsev (Equal), Michael P. Diamond (Equal). Writing – original draft: Dmitri Dozortsev (Equal), Michael P. Diamond (Equal). Writing – review & editing: Dmitri Dozortsev (Equal), Michael P. Diamond (Equal).